“New beginnings are often disguised as painful endings.”
– Lao Tzu
Headaches Due to Low Cerebral Spinal Fluid Volume
While chronic headaches are a common problem usually attributed to migraine and muscle tension, there is another less frequent cause of headaches that is gaining more recognition: headaches related to a low volume of cerebrospinal fluid (CSF). CSF is a clear fluid manufactured in the brain that circulates around the brain and spinal cord that provides metabolic support as well as physical protection against the trauma of daily activities. It is the fluid acquired for testing when a “spinal tap” is performed.
Headaches attributed to low volume of CSF are also commonly referred to as “spontaneous intracranial hypotension” because the headaches are most often, but not always, associated with low CSF pressure. Other names addressing this condition include low pressure headache, and CSF hypovolemia.
Fortunately, while establishing a diagnosis may not always be straightforward, treatment is generally safe and successful, often leading the patient back to a marked improvement or resolution of their chronic headaches.
Scroll down…
Definitions and Terms Related to Pain
Key to Links:
Grey text – handout
Red text – another page on this website
Blue text – Journal publication
.
Headaches due to Low Cerebral Spinal Fluid Volume (CSF)
CSF is normally retained in the central nervous system within the outermost fibrous sheath that surrounds tje brain and spinal cord, the dura mater”, or “dura.” If a leak develops in the dura either related to direct trauma or spontaneously, the loss of CSF results in acute or chronic headaches along with a multitude of non-specific symptoms. In the absence of an acute, identifiable traumatic event, chronic headaches related to CSF leakage can be much more difficult to identify, especially when they appear to occur spontaneously. To make this diagnosis a careful history and assessment must be made to identify people at risk and look for findings that raise significant suspicion enough to warrant obtaining definitive testing to establish the diagnosis.
Clinical Presentation – Symptoms
Orthostatic (Positional) Headache.
The classic pattern of headache due to low CSF volume is orthostatic, meaning the headache worsens when sitting or standing up and relieved when lying flat. Acute headaches from spinal fluid leaking out the puncture subsequent to a spinal tap is not uncommon and is usually temporary. When acute, such a headache generally occurs or worsens within 15 minutes of assuming the upright position but in some patients the lag period may be as long as several hours. When the condition is chronic, however, the headache worsening may not develop for many hours, late into a day or after prolonged standing or walking, before the headache manifests or worsens. The severity and timing of the headache may be related to the size of leak(s) which may be intermittent, simply a “weeping” leak or large and continuous.
Improvement of the headache after lying down is less variable but usually occurs within 15 to 30 minutes. The headache may be diffuse or localized to the frontal, temporal, or most commonly the occipital or suboccipital regions. The headache may be throbbing or nonthrobbing and is rarely unilateral. Some people describe their headaches like the feeling of “an ice cube in an empty glass” or a “pulling sensation from my head down to my neck,” which may offer a clue to the diagnosis.
Headache Severity
The severity of the headache is widely variable; many mild cases probably remain undiagnosed, whereas other people are incapacitated and unable to tolerate activity while upright.
Other Symptoms associated with Low Volume CSF
- Nausea, usually severe, sometimes in the absence of headache
- Tinnitus or ringing in the ears
- Vertigo
- Hearing changes
- Visual impairment
- Neck pain and/or neck stiffness
- Fatigue
- “Brain fog” or impaired short term memory or attention span
- Postural tachycardia (rapid heart rate)
- Postural syncope (loss of consciousness)
Causes and Risk Factors
Headaches due to CSF leaks are not just causally related to postdural punctures from spinal taps, complications related to epidural injections or placement of spinal cord stimulators, there are many circumstances related to spontaneous CSF leaks leading to headaches. In addition, there are often substantial differences in the clinical features, response to treatment, and outcome between the two. In spontaneous CSF leak, the dural defect responsible for the leak is often not a simple hole or rent and may not be associated with a history of trauma or instrumentation.
In fact, the development of spontaneous CSF leaks is likely to be multi-factorial. A common factor is trauma, either recent or in the distant past. . Cervical “whiplash” injuries or back and head trauma may contribute to tears.
Predisposing factors include conditions associated with disorders or abnormalities of connective tissues. People with hyperflexible joints such as those with Ehlers-Danlos and those who are particularly tall, especially those with Marfan’s Syndrom are at increased risk. Those with other, less well-defined variants in musculoskeletal structures such as Chiari malformations, scoliosis and pectus excavatum may be at increased risk.
Screening
An effective screening tool to identify those with headaches due to low CSF volume is the 48 hour leak test.
48 Hour Leak Test:
Purpose:
To determine if the headache has a “postural component”, in which symptoms improve or worsen in response to prolonged changes in body position (horizontal vs vertical).
Rationale:
New spinal fluid leaks often create a unique set of symptoms in which the head hurts when a patient is upright but within 2-30 minutes after laying flat the head pain subsides. However, with chronic leaks many patients need to spend up to 48 hours to tell if position makes a big difference in their pain.
Method:
Spend 48 flat in bed positioned with your head no higher than your hips. That means no pillow when you are on your back, but you can use a pillow when laying on your side. Sitting up even a little will produce contradictory results. Eat in bed and only get out of bed to urinate and then get back in bed.
Patients usually do this in the following way:
- Friday night get in bed.
- Saturday morning get up and go to the bathroom then get back into bed
- Continue in bed until Sunday night.
- On Sunday night before getting out of bed assess your symptoms:
1. Are your head pain, neck pain, neurologic symptoms better, worse, or the same than typical Sunday night?
2. Does this change within 1-2 hours after getting out of bed on Sunday night?
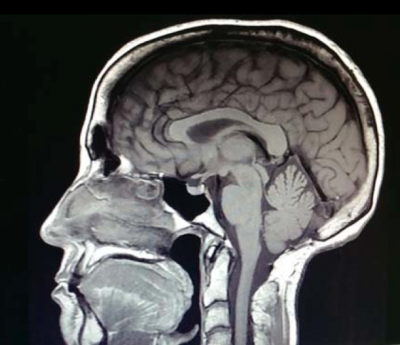
Imaging
MRI of the Brain with Contrast (gadolinium)
Findings on the brain MRI suggestive of low volume CSF:
SEEPS:
- Subdural hematoma (collection of blood under the dura)
- Enhancement of meninges with the contrast
- Enlargement, distension of veins
- Pituitary gland enlargement
- Sagging, low lying cerebellar tonsil, small 4th ventricle
CT Myelogram of the Spine
- Degenerative changes disproportionate for age, such as multiple bulging discs, bone spurs
- Contrast in neural foramen
- Bone spurs against dura
- “Perineural cysts” – thecal aneurysms?
- Tarlov cysts
- One spinal level with subtle differences from others
Radioisotope Cisternography
- Failure of the tracer to reach the brain
- Early filling of bladder with radionuclide (<6 hours)
References
Low CSF Pressure Headaches – Overview
- Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension – 2006
- Spontaneous CSF Leaks Low CSF Volume Syndromes – 2014 Mokri review
- Chronic headache from pdp – post-dural puncture – 2012
Low CSF Pressure Headaches – Treatment
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices
.