“In the face of excruciating pain and uncertainty, I never lost hope, and it never occurred to me to stop fighting – not ever”
-Farrah Fawcett
Pancreatitis Pain
See also:
Treating Pancreatitis Pain:
Medications:
Medications for Pain – Overview
NSAIDs (Non-Steroid Anti-Inflammatory Drugs)
Gabapentin (Neurontin) & Pregabalin (Lyrica)
Integrating the Management of Visceral Pain:
Integrative & Complementary and Alternative Medicine (CAM)
Mindful Intervention
Cognitive Behavior Training (CBT)
Meditation & Mindful Exercises
Physical Intervention
Treatment Recommendations for Managing Pain Associated with Chronic Pancreatitis
Definitions and Terms Related to Pain
Key to Links:
Grey text – handout
Red text – another page on this website
Blue text – journal publication
.
Pancreatitis
Pain generated from the pancreas is generally associated with acute pancreatitis, chronic pancreatitis and pancreatic cancer. Although acute pancreatitis (AP) and chronic pancreatitis (CP) are often thought of as distinct entities, the current belief is that AP often progresses and recurs (recurrent AP or RAP), and ultimately progresses into chronic pancreatitis, essentially representing a disease continuum rather than three separate conditions. While the manifestations of pancreatic pain associated with these conditions have a great deal in common, for the purposes of this section the focus is on the pain of chronic pancreatitis.
Diagnosis of Chronic Pancreatitis (CP)
CAT scans are the preferred initial diagnostic test for CP. The sensitivity of CAT scans exceeds that of ultrasound, (75%–90% vs 60%–70%) although the specificity is similar (CT 85% vs ultrasound 80%–90%). MRIs of the pancreas may be used to provide detailed ductal and cyst assessment and benefits from lack of the radiation exposure associated with CAT scans. Endoscopic ultrasound (EUS) is also a highly sensitive method for diagnosing CP using certain criteria characterising parenchymal and ductal disease.
Causes of Chronic Pancreatitis
Traditionally, the etiology of CP has been individually classified as alcoholic, hereditary, obstructive, due to hyperlipidemia, or idiopathic (a collective category of unknown causes). It is more accurate however to consider that in most cases more than one “etiology” is presen
t. Rather, pancreatitis is based in certain risk modifiers that interact to produce pancreatic disease: toxic-metabolic, idiopathic, genetic, autoimmune and obstructive factors. In the setting of pre-existing risk factors (genetic, metabolic, and environmental), an initial first episode of AP may either lead to complete recovery, or may pathologically progress to recurrent then chronic pancreatitis. It is estimated that approximately 20% of patients with AP have a recurrence and 36% of those patients with recurrence go on to develop CP. Even though excess alcohol intake is
a major risk factor for CP, only about half of patients with CP have alcohol as a cause.
Chronic pancreatitis (CP) is characterized by the progression of inflammation, fibrosis, and scarring of the pancreas which results in loss of function. The pancreas provides two basic functions: exocrine – the production of enzymes necessary for healthy digestion of food and endocrine – the production of insulin, a major hormone that regulates the metabolism of carbohydrates, fats and protein by promoting the absorption of glucose from the blood into liver, fat and muscle cells.
The cascade of events leading to CP is triggered by ongoing damage to the pancreas by repeated episodes of acute inflammation associated with oxidative stress, the build-up of free radicals produced by the exposure and metabolism of alcohol, tobacco smoke and other dietary toxins. As part of the inflammation process, nerves are exposed to biochemical agents that are released following tissue damage, such as H1, K1, bradykinin, ATP, prostaglandins, Substance P (SP), calcitonin gene–related peptide (CGRP), and neurokinins. These inflammatory molecules activate mast cells and platelets which release serotonin (5-HT), nerve growth factor, and histamine, which again activate the sensory nerves.As the cascade of inflammation leading to fibrosis and scarring evolves, the result is pancreatic dysfunction characterized by the impaired production of pancreatic digestive enzymes and insulin.
This pancreatic insufficiency of digestive enzymes (pancreatic exocrine insufficiency or PEI) leads to further complications by impairing adequate digestion and absorption of ingested food, thus causing even greater deficiencies of nutrients including Vitamins A, D, E and K, and antioxidants resulting in malnutrition. The impaired endocrine production of insulin resulting from the inflammation and scarring of the pancreas leads to diabetes.
Diabetes secondary to pancreatic disease is referred to as pancreatogenic diabetes or type 3c diabetes mellitus (DM). More than half of all patients with CP develop diabetes due to the loss of complete islet cell mass, not just beta cells as in type 1 DM, or due to insulin resistance as in type 2 DM.
Symptoms of Chronic Pancreatitis
The classic symptom of CP is severe, dull pain in the mid-upper abdominal (epigastric) area which may radiate to the back and flanks and often worse after eating and exhibits episodic flares. The episodes of pain and their duration vary but tend to intensify as the disease progresses. Pancreatic pain shares many typical clinical characteristics of visceral (organ) pain which are:
- The pain is not always simply or directly linked to morphological changes of the diseased organ;
- Pain may be diffuse and poorly localized;
- The pain may be referred to other locations;
- The pain is accompanied by motor and autonomic reflexes (vomiting, nausea and muscle tension)
The symptoms of CP can develop insidiously and may be challenging to diagnose especially in the early phases. Other symptoms include weight loss and loose stools but these are non-specific and can overlap with other conditions. The loose stools of pancreatitis are often especially foul smelling (steatorrhea) due to the presence of undigested fat resulting from the loss of digestive enzymes due to pancreatic exocrine dysfunction.
Understanding the Pain of Chronic Pancreatitis
Traditionally, the mechanisms thought to be responsible for chronic pancreatitis pain were structural abnormalities of the pancreas. Three underlying mechanisms for structure-related pain include:
(1) Inflammation of the pancreas;
(2) Increased pressure within the pancreatic tissues leading to impaired blood flow and tissue death, and/or related to pancreatic duct obstruction from strictures or stones;
(3) Complications within and/or surrounding the pancreas including formation of pseudocysts, blood clots in local vasculature, scarring causing strictures of the bile duct or development of duodenal or peptic ulcers).
The range of symptoms from pseudocysts is wide-from asymptomatic to severe abdominal pain dependent on its location and size. The clinical presentation of duodenal and bile duct obstruction is variable and can be asymptomatic. Postprandial abdominal pain, early satiety and nausea are the most common symptoms of duodenal obstruction, while pain and abnormal liver function tests are suggestive of bile duct stenosis and cholangitis.
However, these three mechanisms do not entirely explain the intense pain of CP or why there can be a discrepancy between the level of pain and the degree of structural abnormalities, especially when only few structural abnormalities of the pancreas can be identified. For example, numerous studies now indicate that the complications of CP including pancreatic duct obstruction, pseudocysts, bile duct obstruction and duodenal obstruction often do not correlate well with pain.
Ultimately, the pain of CP is multi-factorial, often including more than a single mechanism of pain as well as a complex interaction between structural changes of the pancreas and neurobiological mechanisms in the peripheral and central nervous system. Because the mechanisms responsible for pain in CP are highly variable in the individual patient, there is no single approach that is effective for a
ll patients.
Neuropathic Pain
Recent research indicates a major contributor to CP pain is neuropathic (nerve-based) and the evidence indicates that the neurological changes in CP better correlate with the pain of CP. The pancreas is innervated by two groups of afferent fibers: branches of the abdominal vagus nerve; and fibers that run through the celiac plexus and reach the lower thoracic segments of the spinal cord via the splanchnic nerves. The latter group is best known for stimulating visceral pain.
The primary pancreatic pain receptors have nerve bodies within the dorsal horn of the spinal cord that communicate with second-order nerves within the spinal cord and brain. After the primary sensory neurons are activated such as by alcohol or toxins, neurotransmitters (glutamate, substance P, calcitonin-gene-related-peptide (CGRP) and nitric oxide synthase (nNOS)) are released by the primary nerve endings located in the pancreas, where they act as inflammatory mediators that create pancreatic inflammation characterized by vasodilation, edema, and infiltration by cytotoxic T-lymphocytes, macrophages and mast cells. This process is also known as neurogenic inflammation.
In a recent 2019 study, the four major nociceptive neuropeptides/neuroenzymes in pancreatic nerve cells were evaluated, including substance P, calcitonin-gene-related-peptide (CGRP), vasoactive intestinal peptide (VIP), and neuronal nitric oxide synthase (nNOS). It was found that only increases in the amount of nNOS in pancreatic nerves of CP patients correlated with pain severity. Mechanistically, nNOS upregula- tion is induced by tryptase that is secreted from perineural mast cells in CP tissues. Furthermore, inhibition of nNOS was proposed to inhibit pancreatic pain.
The degree of mast cell infiltration in particular appears to correlate with the degree of neuropathic pain in CP which suggests possible treatment interventions directed at the suppression of mast cells.
(See Palmitoylethanolamide/PEA).
Development of chronic pancreatic pain is thought to result from the structural changes that develop in the pancreatic nerves as a result of neurogenic inflammation. These changes include increased nerve density, hypertrophy, and fibrosis (scarring) which leads first to a localized condition of pancreatic neuropathy. The severity of pancreatic neuritis has been shown to have a major correlation to the severity of abdominal pain in CP.
Pain Sensitization
These structural changes of pancreatic nerves in turn induce functional changes of increased excitability and hypersensitivity of the nerves, termed “peripheral sensitization.” This peripheral sensitization is associated with upregulation of bioactive chemicals such as nerve growth factors, brain-derived neurotrophic factors and proinflammatory cytokines, that lead to increased intensity of pain sensation.
The increased pain signals from the pancreas in turn induce structural and functional changes in the nerves of the spinal cord and brain that affect the processing of pain perception. The result is increased reactiveness of pain-transmitting nerves causing hyper-responsiveness to sensory stimuli and hypersensitivity to pain, termed “central sensitization.”
There are nerve pathways that descend from the brain down the spinal cord (termed “descending pathways”) that suppress or enhance pain signals from ascending the spinal cord to the brain pain centers that determine the experience of pain. These descending pathways act through the release of several mediators, including endogenous opioids, noradrenaline (norepinephrine), serotonin (5-HT) and γ-aminobutyric acid (GABA), which modulate the transmission between primary nerves from the pain source and the secondary neurons in the dorsal horn of the spinal cord that communicate with the ascending nerve pathways to the brain.
The balance between these pathways ultimately determines the quality and strength of the nerve signals entering spinal transmission and processing in the brain. Alterations in the balance of descending modulation from inhibition towards facilitation have been implicated as key to the transition of acute into chronic, neuropathic pain. Experimental evidence suggests that effective activity of inhibitory descending pathways could protect against the development of chronic pain. This argues for focusing early treatment directed at maintaining activity of the inhibitory descending pathways as a means of reducing the risk of having acute pain transition to chronic pain.Thus these pathways are important targets for medications used to treat chronic pain, including certain antidepressant and opioid medications.
The combination of the changes related to the descending pathways and pain sensitization leads to an increase in pain perception and magnification of the pain experience that manifest as the hallmarks of pain sensitization: hyperalgesia and allodynia.
Hyperalgesia
Hyperalgesia is an exaggerated, increased painful response to a stimulus which is normally painful. Hyperalgesia often accompanies visceral pain syndromes and can be a consequence of central sensitization.
Allodynia
“Allodynia” is when a stimulus that is not normally painful, such as normal physiologic stimuli, is experienced as painful.
Thus, peripheral and central sensitization associated with CP contributes to a complex pain syndrome involving not only the pancreas, but also the nervous system. As the pain system sensitizes, it can ultimately become an autonomous and self-perpetuating pain state that is independent of the original source of pain. Pain sensitization is shared by many other chronic abdominal pain conditions including irritable bowel syndrome, ulcerative colitis, endometriosis and interstitial cystitis.
It is recognized that ongoing pain may induce altered central pain processing, e.g., central sensitization or pro-nociceptive pain modulation. When this is present conventional pain treatment targeting the nociceptive focus, e.g. opioid analgesia or surgical/endoscopic intervention for CP or other chronic pain conditions, often fails even if technically successful. It should also be noted that pain sensitization, peripheral and central, likely develops in many if not most chronic pain conditions including headaches, neck and back pain, arthritis. In fact, the central sensitization process includes other aspects of disease processes in addition to pain. Chronic non-pain conditions with different aspects of a central sensitization process include chronic fatigue syndrome, PTSD and restless leg syndrome. See list of conditions associated with central sensitization.
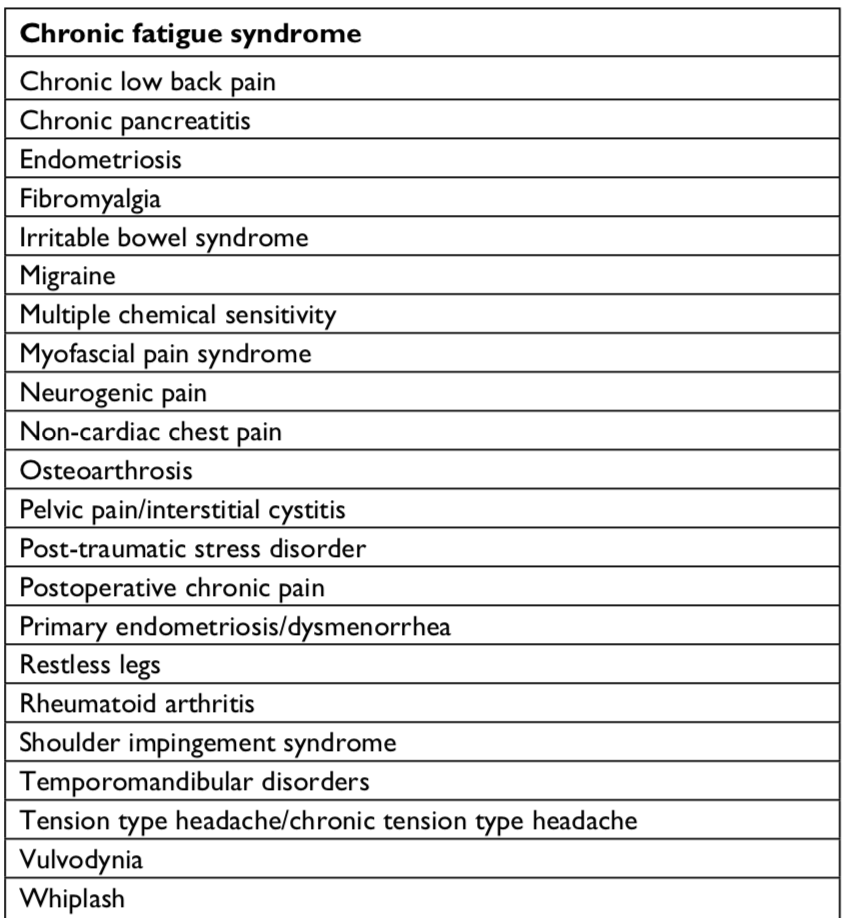{kind=link}
As a consequence of altered central pain processing associated with sensitization, conventional pain treatment such as opioid analgesia or surgical/endoscopic procedures often fail even if technically successful. Current research emphasizes the need to treat pain sensitization to achieve the greatest success for managing the pain of chronic pancreatitis. The treatment of the neuropathic pain associated with sensitization is a major focus of contemporary pain management and includes prescription medications and non-prescription nutraceutical supplements as well behavioral practices.
Treating Pancreatic Pain
The management of chronic pancreatic pain is best achieved by a multi-disciplinary approach, including the expertise of the gastroenterologist, surgeon, interventional pain specialist, medical management pain specialist and nutritionist. Inter-disciplinary referrals to assess different treatment options provides the patient with the most comprehensive approach to successfully manage CP pain.
The first step in treating CP pain is conservative therapy, including lifestyle management (e.g., stopping smoking and discontinuing use of alcohol), dietary approaches, treatment directed at central sensitization and pain medications. When pain persists despite these measures, endoscopy may be indicated when necessary, for example, to treat blockage of the pancreatic duct. As a last resort, surgical procedures such pancreatic resection may be warranted when endoscopy fails.
Dietary Approaches in CP Pain
Dietary patterns play significant roles in chronic pain for many conditions including CP. Evaluating diffeerent diets and nutrients and the roles they play in chronic pain is beyond the scope of this page. (See Diet and Diets). However, a few key points need to be made to underscore the importance of diet in chronic pain, including CP.
The Western diet based on processed meat, sugary foods, refined grains, and low intake of fruits and vegetables causes an excessive production of proinflammatory mediators that sensitize nerves and also causes fewer anti-inflammatory mediators, including antioxidants and antioxidant defense. The western diet does not necessarily increase inflammation directly but it does induce a reduction in anti-inflammatory defenses and contributes to chronic pain. Reduction of chronic pain can be obtained by reducing the intake of proinflammatory foods and increasing the intake of unsaturated fats, fruits, and vegetables. Diets rich in whole-grains, fish, fruits, green vegetables, and olive oil help reduce oxidative stress, an important contributor to CP.
In addition to what one eats, and how much, when one eats may also impact chronic pain, inflammation and oxidative stress.
Caloric Restriction and Fasting
Therapeutic fasting techniques include intermittent fasting (e.g., 60% energy restriction every other day), partial fasting (e.g., 5-day diet providing 750–1100 kcal), and time-restricted feeding (limiting the daily period of food intake to ≤8 h). Therapeutic fasting not only leads to weight loss, but also reduces the proinflammatory state and oxidative stress. Intermittent fasting (IF) can decrease the pain experience through reduction in central and peripheral inflammation, reduce oxidative stress and decrease peripheral and central sensitization.
See: Diet and Fasting
Endoscopic Management of CP
Endoscopic interventions are generally performed for pancreatic duct strictures and pancreatic duct stones. Endoscopic therapy can be used to dilate strictures with insertion of stents that provide pain relief in up to 89% of patients. For those patients with CP complicated by biliary obstruction, which occurs in 3%–23% of patients, ERCP treatment for biliary strictures with stents is effective. Additionally, small stones in the main pancreatic duct can be removed with endoscopic retrograde cholangio-pancreatography (ERCP) although stones ≥ 5mm may require lithotripsy.
Surgical Management of CP
dures may
preempt the development of extensive structural changes and limit the development of pain sensitization discussed above.
Surgical treatment may indicated for:
- Intractable treatment-resistant pain
- Small duct disease
- Enlargement of pancreatic head
- Failure of previous drainage procedures
- Suspicion of malignancy
- Chronic narcotic dependence
- Impaired quality of life
- No reversible cause of chronic pancreatitis,
- Unresponsiveness to maximal medical, endoscopic and sometimes surgical therapy and
- Adequate islet cell function (non-diabetic).
Exploring surgical procedures and their specific indications is beyond the scope of this site and the reader is referred to the surgeons to further explore this topic. Please note there are downloadable publications regarding surgery in CP in “References” at the bottom of this page.
Interventional Management of CP
Celiac Plexus Blocks
Pain signals from the pancreas are sent to the celiac plexus nerves where they converge at T12-L1 vertebral levels, via the sympathetic nervous system and relayed through the celiac plexus to the splanchnic nerves. Endoscopic ultrasound-guided celiac plexus nerve blocks with steroid and a local anesthetic (bupivacaine) have been shown to be effective in just over half (55%) of patients with CP, but their duration of benefit is limited, lasting only days to weeks, so repeated procedures are required.
Celiac plexus neurolysis (CPN) or ablation provides more prolonged benefit by the injection of alcohol or phenol but may be associated with more complications including postural hypotension and diarrhea. Endoscopic guided celiac plexus neurolysis procedures have previously been widely used for pain in CP but is now considered obsolete by some specialists due to poor long-term outcomes and risk of side effects.
Splanchnicectomy
Pain signals can also be interrupted at the level of the splanchnic nerves. Splanchnicectomy consists of sectioning the roots of the splanchnic nerves from T5 to T10 via a thoracoscopic procedure. Partial to complete relief has been noted with thoracoscopic splanchnicectomy, but analgesic effects last for only 2 to 3 months. Bilateral thoracoscopic splanchnicectomy have been performed often in the past, but again offer short-term benefits only so these procedures are only indicated in selected cases. The use of nerve blocks for the management of intractable abdominal pain are offered by interventional pain management specialists.
When hyperalgesia and central sensitization is well established in CP, the pain experience can become independent of the local pancreatic nerve drive and consequently denervation of peripheral nerves become ineffective. This is the argument for failed splanchnicectomy procedures that while procedurally successful nevertheless fail to provide pain benefit. This finding in visceral pain syndromes such as CP contrasts with somatosensory disorders, such as painful polyneuropathy, where regardless of signs of central sensitization, a primary afferent input is critical for maintaining ongoing and evoked neuropathic pain. In these cases the effectiveness of topically applied drugs supports that peripheral pain-generating mechanisms are key to maintain central sensitization and hyperalgesia.
Spinal Cord Stimulators (SCS)
Research suggests that spinal cord stimulation suppresses visceral hyperalgesia and studies of spinal cord stimulation in patients with chronic pancreatitis have demonstrated significant pain relief. The use of spinal cord stimulators may represent a useful therapeutic option.
A recent 2019 study evaluated supplementing SCS treatment with duloxetine (Cymbalta) concluded at 1-year follow-up that patients receiving duloxetine and SCS had better pain relief than those receiving SCS alone. This contrasted with patients receiving pregabalin or gabapentin with SCS who did not have significantly more pain relief than patients receiving SCS alone.
Pharmacologic Management of CP
NSAIDs (Non-Steroid Anti-inflammatory Drugs)
While some visceral pain may respond well to NSAIDs, especially menstrual pain, NSAIDs are usually ineffective or counter-productive in gastrointestinal disorders such as inflammatory bowel diseaes and interstitial cystitis, cau
sing increased pain and relapse.
Opioids
When initial treatment with non-opioids is inadequate, it is often necessary to turn to opioids. While there is incomplete research to identify specific opioids as being more preferable than another at this point in time, there are some principal recommendations to be made. Because of the significant likelihood of the need for long-term use of opioids once the pain is severe enough to mandate their use, the choice of opioid should take into account the potential for the opioid’s development of tolerance. Safety cautions should also bear on the opioid’s risk for abuse and potential for overdose. Finally, there is limited research available suggesting some opioids are more effective for pancreatic pain than others.
Buprenorphine (Belbuca, Butrans)
Traditional opioids may cause spasm of the sphincter of Oddi which causes increased biliary tract pressure and may contribute to the abdominal pain of CP. The spasm effect seems to be related to the dosage and plasma concentration of the opioid.
Buprenorphine is a unique opioid recently introduced into pain management. It offers multiple safety benefits over traditional opioids but in CP it has the unique characteristic of not inducing spasm of the sphincter of Oddi which suggests it may be the initial opioid of choice when introducing opioids for the management of CP pain.
Tramadol
Tramadol offers relatively weak opioid activity but also provides a secondary mechanism of action for pain by increasing noradrenaline and serotonin uptake in the spinal cord. Preclinical testing has shown that μ-opioid activity is primarily responsible for analgesia in acute pain, whereas noradrenaline reuptake inhibition is more important in chronic pain. This dual mechanism of action suggests the likelihood of slower development of tolerance compared with traditional opioids such as morphine that gain their analgesic benefit solely from their effects on the mu-opioid receptor (μ-receptor).
Tramadol’s action on the noradremaline reuptake in the descending pathways also benefits the treatment of pain sensitization as discussed above.
Tramadol is a more potent analgesic than codeine, but generally less potent than morphine at commonly used doses. However, tramadol has been shown to be more effective than morphine in patients with CP, while also showing fewer gastrointestinal side effects compared with morphine for the same level of analgesia. Thus, after buprenorphine, tramadol may be the preferred choice when turning to opioids for CP pain.
Tapentadol (Nucynta)
Tapentadol is a low affinity mu opioid receptor agonist combining μ-opioid receptor agonism and noradrenaline reuptake inhibition (NRI) as a single medication, with both mechanisms contributing to its analgesic effects. NRI activity increases nerve synapse availability of the neurotransmitter noradrenaline (norepinephrine) which produces analgesia through the activation of α2‐adrenoceptors, especially in the descending pain inhibitory pathways described above. Tapentadol provides analgesic benefits by restoring descending inhibitory tone.
As previously noted, a significant component of the pain of CP has been identified as neuropathic (nerve) pain accompanied by peripheral and central sensitization. Our understanding of the mechanisms of pain sensitization suggests that the inhibitory descending pathways play key roles and tapentadol, even more potently than tramadol, acts of these pathways. So, from a mechanistic point of view, tapentadol may offer superior benefits in the management of CP pain by treating both the acute pain but also the pain sensitization that contributes to the magnification of pain over time.
In fact, as noted above, recent experimental evidence suggests that effective activity of inhibitory descending pathways might protect against the development of chronic pain. Thus focusing early treatment directed at maintaining activity of the inhibitory descending pathways may reduce the risk of having acute and/or recurrent pancreatitis pain transition to chronic pancreatitis pain. This argument suggests that tapentadol (and/or possibly duloxetine (Cymbalta) – see below) may be a preferred medication to treat the early pain of pancreatitis.
Additionally, tapentadol shows minimal serotoninergic activity. This pharmacological profile may be important because the activation of serotoninergic descending pathways are excitatory and produce pain-promoting effects as well as stimulating nausea and vomiting. Other opioids known to have serotonergic effects include tramadol, oxycodone, codeine, fentanyl and methadone.
In clinical trials in patients with chronic pain, it has been shown that the efficacy of tapentadol is greater than tramadol, similar to that of oxycodone, but it produced significantly fewer gastrointestinal side-effects and treatment discontinuations. While studies are lacking that specifically assess long term management of CP with tapentadol, a case report published in 2017 demonstrated significant effectiveness that persisted more than three months with no apparent analgesic tolerance buildup. In this study, the dose of tapentadol was 50 mg in the morning and 100 mg in the evening.
An important principle governing treatment of chronic pain is to use a multi-modal approach. In other words, treat pain with medications or other modalities that work through different mechanism in order to achieve either synergistic or supplementary analgesic benefits. In addition, engaging multiple mechanisms with combination therapy may not only provide superior analgesia but agents may also be used at lower doses such that the adverse side effects associated with each drug are minimized.
A 2018 animal study evaluated the combinaton treatment of central sensitization pain in osteoarthritis with both tapentadol and pregabalin (see “Gabapentenoids” below). In this case, tapentadol provides analgesic benefit via action on both the mu-opioid receptor and the descending pathway while pregabalin suppresses spinal nerve hyperexcitability, providing superior analgesia.
See: Tapentadol (Nucynta)
Oxycodone
Oxycodone is generally effective for managing CP pain and research suggests that it is superior to morphine in this regard. This may be due to oxycodone’s activity at the kappa-opioid receptor (κ-receptor), a unique activity that sets it apart from other commonly used traditional opioids. Limited studies suggest that activation of the κ-receptor may be particularly effective for reducing visceral pain.
On the downside, anecdotal evidence suggests that oxycodone may be more likely to be abused and may develop tolerance more quickly than other traditional opioids.
Levorphanol
Levorphanol is a potent opioid that offers greater efficacy than morphine at the mu-opioid receptor. It also offers dual mechanism analgesic activity that is different from either tramadol or tapentadol. In addition to potent mu-opioid activity directed at acute pain, levorphanol also provides potent NMDA antagonist activity unlike traditional opioids. Antagonism of NMDA is believed to offer benefit in pain sensitization and neuropathic pain, making levorphanol a potential treatment preference over traditional opioids and one potentially more potent than tapentadol and oxycodone.
See: Levorphanol
Neuromodulators
The term “neuromodulator” has been applied to a number entities. In its use here, the term “neuromodulator” refers to a medication or supplement that impacts nerves, or the nervous system, in such a way as to modulate or change their function – in this case to modulate neuropathic pain.
Neuromodulators – Gabapentinoids
Treatment with the gabapentinoids, gabapentin (Neurontin) and pregabalin (Lyrica), has been shown to be helpful in patients with pain due to CP, especially those with central sensitization. There are multiple mechanisms by which these agents work in neuropathic conditions, but an important mechanism is likely a reduction in pain hypersensitivity of nerves in the central nervous system (CNS), brain and spinal cord.
The gabapentinoids bind to the α2δ1 subunit of voltage‐gated calcium channels (VGCCs) and inhibits calcium currents and the release of neurotransmitters in nerves, allowing it to modulate dysregulated neuronal signals.
One technique that may allow identification of a CP patient with central sensitization and greater potential for responding to the gabapentinoids is to test for hyperalgesia in the T-10 dermatome (where neuronal afferents from the pancreas and somatic tissue converge). Those with evidence of hyperalgesia here have a higher likelihood for effective treatment response to the gabapentinoids.
A 2012 evaluated the benefit of pregabalin for pain in patients with CP and central sensitivity. The study assessed doses ranging from 75 mg to 300 mg twice a day for 3 weeks and concluded that pregabalin provided moderate antihyperalgesic effect, compatible with a reduction of central sensitization. However, the benefit was found only in areas distant from referred pancreatic area and was more pronounced in skin than in deeper tissues. The overall conclusions of the study was that pregabalin modestly reduces the spreading hyperalgesia as a smanifestation of central sensitization associated with chronic pancreatitis pain. This effect was evident after three weeks of pregabalin treatment and was most evident for electric skin pain thresholds.
A 2016 study evaluated narcotic naïve patients with chronic calcific pancreatitis with pain recurrence for 2 months following pancreatic ductal clearance of stones. The study found the combination treatment of pregabalin and antioxidants provide significant relief of CP pain.
This study was supported by a 2018 animal study of osteoarthritis evaluating central sensitization treatment with the combination of pregabalin and tapentadol.
In this 2018 study, the combination treatment with tapentadol and pregabalin restored descending noradrenergic inhibitory tone and also inhibited nociceptive transmission at the level of the spinal cord. This significant study demonstrated that pregabalin and tapentadol, targeting different mechanisms of centrally driven chronic pain associated with osteoarthritis, when administered together can restore descending inhibitory tone and also reducing spinal neuronal hyperexcitability. and may therefore provide superior analgesia.
Neuromodulators – Antidepressants
Benefit from antidepressant drugs has been found in CP, especially those from the SNRI class, such as Duloxetine (Cymbalta), which have less side effects than tricyclic antidepressants. The SNRI antidepressants act on the serotonergic and noradrenergic systems in the descending pathways described above and facilitate inhibition of pain signaling in the brain and spinal cord. A 2019 study demonstrated that supplementing spinal cord stimulator (SCS) management of CP pain with duloxetine improved pain control compared with SCS alone.
Tricyclic antidepressants such as amitriptyline (Elavil), desipramine and doxepin have also shown effectiveness for visceral pain, but treatment should be initiated with low doses to avoid side effects such as drowsiness and dry mouth. In visceral pain syndromes accompanied by anxiety and/or depression, visceral pain has also been shown to respond to SSRIs such as fluoxetine (Prozac) and citalopram (Celexa).
Antioxidants
The most recent systematic reviews and meta-analysis studies, published in 2013 and 2015, together support the conclusion that antioxidants are useful for CP-induced pain. In the West, alcohol abuse is the most common cause of CP, which accounts for 70% of cases. But the second most common cause, idiopathic chronic pancreatitis, also known as tropical pancreatitis, has a quite different clinical history from other kinds of pancreatitis.
Studies of combined antioxidant therapy for the 2 types of patients with CP show mixed results for analgesic effectiveness. In addition, the characteristics of patients, like age and gender, may also influence results. For example, a recent study suggests that combined antioxidant therapy may be less effective in more elderly patients who have alcohol as the etiology. Thus, the particular subgroup of patients with CP that may benefit from combined antioxidant therapy needs further study. Furthermore, the optimal combinations and dosing of antioxidants remain to be defined.
Many studies about antioxidant therapy for reducing pain induced by CP have been completed, but most of them were single antioxidant trials evaluating antioxidant supplements that included selenium, β-carotene (vitamin A), vitamin C, vitamin E, methionine, allopurinol, dimethyl sulfoxide (DMSO), SAMe, and curcumin, the active constituent of turmeric. The 4 most commonly studied antioxidants in pancreatities are selenium, β-carotene, vitamin C and vitamin E. But most of the single antioxidant studies demonstrated disappointing results for pain relief, leaving the question of efficacy of sole antioxidant agent controversial.
However, when one focuses on the combined antioxidant trials including systematic reviews and meta-analysis, a strong association of combination antioxidants for pain in CP is observed. Additionally, combination antioxidant therapy is safe with no serious adverse identified.
Dhingra et al, 2013
In this study, a combination of antioxidants including organic selenium Yeast (600 ug), vitamin C (540 mg), Vitamin A (β carotene – 9000 IU), vitamin E (270 IU), and methionine (2 g) demonstrated improved pain with reduced number of painful days per month and reduced amount of pain medications needed.
Shah et al, 2010 & Siriwardena et al, 2012
In these studies, for 6 months patients were provided Antox, a specially formulated commercial nutritional supplement designed for use for conditions associated with oxidative stress based on co-factors of the endogenous glutathione peroxidase pathway: selenium, vitamin C (ascorbic acid) and methionine were proposed as key antioxidants.
This supplement contains selenium (from yeast SelenoPrecise® – 300 ug), vitamin C (720 mg), Vitamin E (228 mg) and methionine (2880 mg). The outcome of these studies demonstrated improved quality of life, a reduction of average pain scores and reduced use of opioids and other analgesics.
Bhardwaj et al, 2009
In this study, patients were provided organic selenium Yeast (600 ug), vitamin C (540 mg), Vitamin A (β carotene – 9000 IU), vitamin E (270 IU), and methionine (2 g) for 6 months. There was a reduction in the number of painful days per month and a reduced amount of pain medications needed. Furthermore, more patients became pain free in the antioxidant vs placebo groups. Biomarkers tested reflected reduced levels of oxidative stress in these patients with CP.
Kirk et al, 2006
In this study, patients were provided Antox (at a different dose than the studies noted above) for 10 weeks. This supplement contained selenium (75 mg), vitamin A (β-carotene – 3 mg , vitamin E (47 mg), vitamin C (150 mg), and methionone (400 mg) and was provided 4 times per day. Patients noted improved quality of life and reduced pain.
Antioxidants and Oxidative Stress
A major contributing cause of CP is oxidative stress, whic
h leads to progressive fibrosis accompanied by functional insufficiency and intractable pain. Oxidative stress is an imbalance between reactive oxidative species (ROS – also known as free radicals) and antioxidants in your body. ROS are oxygen-containing molecules with an uneven number of electrons which allows them to easily react with other molecules. ROS are created as normal byproducts of metabolism by cells and are, under normal, healthy conditions neutralized by antioxidants manufactured within cells. When production of ROS exceeds their neutralization by antioxidants, ROS-derived cellular injury can occur which is known as oxidative stress. Levels of these ROS byproducts are increased in chronic pancreatitis.
The theoretic role of antioxidant therapy has been a mainstay for a long time but research remains unclear as to its role in managing CP despite the fact that micronutrient antioxidant therapy for relieving painful CP has been recommended for more than 30 years. The reason for this is likely due to inadequate research, including inadequate assessment of individual antioxidants and inadequate study designs. However, it is expected that continued research will provide solid evidence to justify the usefulness of antioxidative phytoceuticals in the treatment of pancreatitis.
It is also important to consider that due to exocrine insufficiency that often accompanies CP, there is increased risk for impaired absorption of nutrients leading to clinical or subclinical malnutrition. Routine supplementation with antioxidants in this circumstance is certainly reasonable along with careful dietary guidance.
Antioxidants have potential to play a number of roles in CP:
- Reduce the development of fibrosis that leads to obstruction and dysfunction
- Suppressing the progression of acute to chronic pancreatitis
- Reduce the pain associated with CP
- Reduce the risk of progression of CP to pancreatic cancer.
Reduce the development of fibrosis that leads to obstruction and dysfunction
A large study demonstrated that antioxidant supplementation leads to a significant reduction in oxidative stress related to pancreatic fibrosis. Another study investigated 61 patients with CP and showed that the levels of surrogate markers of fibrosis (malondialdehyde, thiobarbiturate acid-reactive substances (TBARS)) were significantly decreased with antioxidant supplementation. The antioxidants used in this study included vitamin C (ascorbic acid), vitamin A (β-carotene), vitamin E (α-tocopherol), organic selenium, and methionine, which also led to significant reduction in pain. EGCG ((-)-epigallocatechin-3-gallate), another antioxidant found in green tea, has also been suggested as potentially effective in CP.
In healthy pancreas, pancreatic stellate cells (PSCs) are inactive and account for only about 4–7% of the pancreas and, in contrast to the more abundant islets or acinar cells that produce insulin and digestive enzymes respectively, PSCs neither secrete hormones nor digestive enzymes. However, in pancreatic ductal adenocarcinoma (PDAC) and chronic pancreatitis (CP), activated PSCs deposit collagen fibers that contribute to the progression of pancreatic fibrosis.
Pancreatic fibrosis is known to be a predisposing condition that increases risk for both chronic pancreatitis (CP) and pancreatic cancer, especially pancreatic ductal adenocarcinoma (PDAC). Because PSCs have a vital role in pancreatic fibrosis, any agents that can suppress the activation of PSCs could have potential as a treatment strategies in CP and PDAC.
Coenzyme Q10 (CoQ10) and Pancreatic Fibrosis
Coenzyme Q10 (CoQ10), known as ubiquinone, is powerful antioxidant in humans and an essential cofactor in mitochondrial oxidative phosphorylation, the process by which energy is produced within cells. CoQ10 has roles in many physiological processes and is beneficial in treating cancers that require chemotherapy and in diseases like statin myopathy, congestive heart failure and hypertension.
A 2017 laboratory study demonstrated that CoQ10 significantly suppressed the activation of PSCs, suggesting that CoQ10 should be an effective approach for pancreatic fibrosis. In this study, CoQ10 also significantly reduced the intracellular level of ROS in PSCs and the down-regulation of intracellular ROS in PSCs may be the underlying mechanism by which CoQ10 suppresses activation of PSCs.
A follow-up 2019 animal study showed that CoQ10 significantly decreased pancreatic fibrosis in a mouse model of CP. These early, preclinical studies strongly suggest potential benefit of supplementing with CoQ10 in CP but human studies need to be completed to confirm benefit and establish doses.
Suppressing the progression of acute to chronic pancreatitis
Animal studies support the effectiveness of antioxidants in reducing the development of fibrosis and inflammation, the hallmarks of CP, but there is a lack of research that demonstrates lessening of progression to CP in human studies.
Reduce the pain associated with CP
The first study to evaluate long-term (10 years) benefit of 30 patients with CP treated with antioxidant therapy, demonstrated relief of pain. However, an additional evaluation (the 2012 ANTICIPATE study) by same research group concluded that antioxidant therapy did not reduce pain in CP caused by alcohol.
However, subsequent meta-analysis and systematic reviews published in 2013 and 2015 concluded, based on current evidence, that oxidative stress plays an important role in the pathophysiology of chronic pancreatitis, and treatment with antioxidants is effective in relieving pain. Antioxidant supplementation may be especially important for chronic pancreatitis patients with low antioxidant capacity in their blood.
In an updated 2015 systematic review and meta-analysis of antioxidant therapy in pancreatitis, multiple benefits were identified:
Chronic Pancreatitis (CP)
In the context of CP, three of four studies reported that antioxidant therapy improved patients quality of life as well as cognitive, emotional, social, physical and role function. Two of three studies showed a significantly shorter hospital stay in the treatment groups. In addition, six of eleven trials reported a reduction of pain.
In studies that assessed laboratory outcomes of antioxidant therapy, eight of nine studies showed a significant decrease in serum free radical activity and a significant increase in serum antioxidant levels. One of two trials reported a decrease in inflammatory biomarkers and one study reported a decrease in the levels of serum amylase.
Acute Pancreatitis (AP)
In the context of AP, one of four studies reported that the mortality rate was reduced following antioxidant therapy. Four of eight studies showed a significantly shorter hospital stay in the treatment groups. Additionally, four of eight trials reported a reduction in complications and organ dysfunction. Three of five studies showed a significant increase in serum free radical activity and a significant increase in serum antioxidant levels. While three of seven trials reported a decrease in inflammatory biomarkers, one trial reported an increase in inflammatory biomarkers. Indeed, three of the five studies demonstrated a significant decrease in CRP levels.
Additionally, a 2016 study found the combination of antioxidants and pregabalin rather than antioxidant alone significantly reduced pain recurrence after endoscopic ductal clearance in CP.
Reduce the risk of progression of CP to pancreatic cancer.
Research regarding the role of antioxidants in cancer prevention have shown that pancreatic cancer risk is inversely associated with total fruit intake, especially in non-smokers, suggesting that antioxidant intake significantly reduces pancreatic cancer risk.
NRF2 Activators and SIRT 1 Activation
Recent research has identified certain processes to be very effective at stimulating our body’s natural mechanisms for creating antioxidants through a process called NRF2 activation. the cells natural response to oxidative stress. NRF2 (nuclear factor erythroid-related factor 2) is a transcription factor that activates over 500 genes via molecules called sirtuins, especially SIRT 1. NRF2 activation can be achieved through exercise, calorie restriction (including fasting) and ingestion of natural nutrients that are NRF2 activators.
Common natural nutrients that are NRF2 activators include curcumin (from turmeric spice – probably the best studied and most potent NRF2 activator), along with resveratol (from grapes), quercitin (from onions) and sulphoraphane (from broccoli) followed by antioxidants found in green tea and other soures. Different nutrients may activate NRF2 by different mechanisms and, when taken together, may be synergistic, or more effective when taken separately.
NRF2 activity modulate numerous processes by controlling gene expression, DNA repair, oxidative stress response and mitochondrial function. Additionally, NRF2 activators may inhibit pro-inflammatory factors derived from macrophages and mast cells.
As such, supplementing with NRF2 activators may offer benefit in promoting an effective response to oxidative stress. In fact, given the belief that the optimal response to pain related to pancreatitis should include efforts to suppress the development of central sensitization. Ideally, this may be considered as the first step to engage at time of the initial bout of acute pancreatitis and maintained to avoid recurremt episodes or evolutiom to chronic pancreatitis.
See: NRF2 Activators
NMDA Antagonists
One of the best characterized mechanisms in the early phase of central sensitization is activation of the N-methyl-D-aspartic acid (NMDA) receptor.
Ketamine
Ketamine has been used traditionally as an anesthetic since in 1965, but currently showing great promise in various chronic pain conditions as well as depression. Ketamine is a noncompetitive NMDA receptor antagonist that blocks the NMDA receptor and has been shown to reverse hyperalgesia and reduce central sensitization associated with CP in an experimental study.
PERT (Pancreatic Enzyme Replacement Therapy)
Due to tissue damage related to CP, patients may be unable to produce adequate amounts of digestive enzymes, termed pancreatic exocrine insufficiency (PEI). Symptoms of PEI include bloating, abdominal pain, diarrhea, especially steatorhea (diarrhea associated with undigested dietary fats and oils that is especially foul smelling), malnutrition, muscle wasting and weight loss that can be profound. Deficiencies of vitamins A, D, E and K are not uncommon in PEI, found in up to 2/3’s of patients with CP. It is recommended that bone density assessment be performed every 1-2 years in all individuals with CP given the high risk for osteoporosis.
Diagnosis of PEI can be confirmed with a stool test, fecal elastase-1 (FEL-1), an indirect test of pancreatic function. FEL-1 measurement is easily performed by collecting a pea-sized amount of feces for analysis. The FEL-1 test has high sensitivity in severe PEI (85%– 100%) but less so in moderate PEI (35%– 100%) and mild PEI (25%–67%), although it has a specificity >93%. It is the most appropriate first line investigation for screening for PEI in patients at risk.
Replacement therapy with pancreatic enzymes (PERT) can be effective for improving the patients nutritional status, reducing weight loss and muscle wasting as well as possibly reducing pain. There are v
arious branded products of pancrelipase (pancreatic enzyme) available, falling into two categories: enteric coated and non-enteric coated. The use of proton pump inhibitors (PPIs) such as omeprazole or H2-receptor antagonists (tagamet) to reduce gastric acid secretion may be necessary to improve absorption, particularly with non-enteric coated products.
The Role of PERT in Reducing Pain
Cholecystokinin (pancreozymin) is a hormone of the gastrointestinal tract that stimulates the digestion of fat and protein. Cholecystokinin (CCK) is synthesized and secreted by cells in the duodenum, the first segment of the small intestine, and stimulates the release of bile from the gall bladder into the intestine and the secretion of digestive enzymes by the pancreas. Patients with CP have been found to have elevated levels of CCK (up to three-fold higher) which is proposed to generate pain by increasing pain in the pancreatic duct and/or by activation of pain receptor pathways in the nervous system.
PERT degrades CCK releasing factor in the duodenum which lowers CCK levels and thereby purportedly reduces CP pain. Only non-enteric coated formulations have duodenal protease activity and research suggests that this type of enzyme formulation improves CP pain. However, most studies using enteric coated formulations (which are not active in the duodenum and hence cannot degrade CCK-releasing factor) do not demonstrate any improvement on CP pain.
Most patients with PEI can be managed with normal diet (30% fat content) and PERT, however if calorie intake is low, protein supplementation should be considered. The recommended starting dose of PERT is 50,000 units with meals and 25,000 units with snacks but this may need to be increased.
Integrative Management – Complementary and Alternative Medicine (CAM) Treatment
There are a number of biological factors that drive the pain sensitization process that occurs in CP. Several candidates have been identified but perhaps the most prominent is nerve growth factor (NGF). This is normally only found in pancreatic islets but with the development of CP, NGF spreads much more widely to the parenchyma in both acini and ducts.
Mast cells
One important cell type that produces NGF is the mast cell, whose numbers are increased in painful but not painless CP. Mast cells are resident immune cells in the GI tract, skin, lung, brain and other tissues and are classically known as mediators of type I hypersensitivity anaphylactic allergic reactions. When mast cells are triggered, they release biochemically active products like histamine, serotonin, cytokines, prostaglandins, etc. Moreover, mast cells maintain a very close spatial association with intra-organ nerves (found sometimes as close as 20 nm away from nerve endings).
Mast cells are also a source of tryptase, which along with trypsin are significant contributors to the pain sensitization process. The biochemical mediators of inflammation such as Substance P can in turn degranulate mast cells causing them to release more biochemical activators of inflammation, leading to a vicious cycle perpetuation of the pain state.
Mast cells have been implicated in the evolution of pancreatic neuritis which is a fundamental component contributing to the development of peripheral and central sensitization which are the driving forces in the pain of CP. Furthermore, the extent of mast cell infiltration into pancreatjc nerves appears to correlate with the severity of CP pain.
It has been proposed that mast cells may be responsible for the induction of peripheral nociceptive sensitization and peripheral neuroplasticity with consequent central hypersensitivity in CP.
See: Mast Cell Activation Disease (MCAD)
Substances that can stabilize mast cells are believed to be beneficial in suppressing the evolution of inflammation and the pain sensitization process. Palmitoylethanolamide (PEA) is a nutraceutical substance with evidence supporting a stabilizing effect on mast cells and has been suggested to be an important means of suppressing pain sensitization. Incidentally, mast cells are also implicated in the process of increased pain related to environmental change such as cold weather and barometric change.
Cannabinoids
Other CAM Treatments
Because visceral pain syndromes and associated pain sensitization, even more than somatic (musculoskeletal) pain syndromes, are strongly impacted by stress, particularly psychological distress, an integrative approach that incorporates means of improving coping skills and reducing stress is a key element to successful pain management. Several approaches have been shown to be effective.
See Using the Mind
Cognitive Behavioral Therapy (CBT)
Cognitive behavioral therapy (CBT) teaches people to recognize the relationship between thoughts, feelings, and behaviors. The goal of CBT is to train an individual to examine his or her negative cognitions (thought patterns), understand how they may impact his or her behavior and emotions, and ultimately work to change maladaptive or detrimental thought patterns. Typical CBT counsel
ing interventions are brief, lasting from 4 to 12 individual or group sessions. A downloadable introductory course in CBT is also available.
See Cognitive Behavioral Therapy (CBT)
Hypnotherapy, or the use of medical hypnosis, includes techniques that can be easily learned and very effective in reducing stress and it’s impact on pain and other symptoms related to visceral pain syndromes. Hypnosis is an increasingly used technique for control of chronic pain. Hypnosis modulates the pain experience by creating a functional disconnection between the prefrontal cortex, the center of decision making and the anterior cingulate, which is involved with attention and motivation.
See Hypnotherapy
Stress management is particularly important in the management of most visceral pain syndromes.
Diet Considerations
Diet clearly plays a role in the management of most visceral pain syndromes, particularly IBS, Crohn’s and Ulcerative Colitis, but also in Interstitial Cystitis. The specifics of dietary management of these individual conditions is deferred to sections focusing on the individual diagnoses but of interest are the emerging concepts of the gut microbiome and of “leaky gut syndrome.”
The Gut Microbiome
The term “microbiome” was originally used to refer to the collection of the genomes (genetic materials) of the microbes in a particular ecosystem, in this case the gut. The term “microbiota” was originally used to refer to the actual organisms. These terms are now used somewhat synonymously, although not correctly. The intestines, or gut, contains trillions of microbes, mostly bacteria, and the balance of different species is believed to influence the health of an individual as well as to impact the integrity of the lining of the gut.
Probiotics
Probiotics are live microorganisms that are used as non-digestible food ingredients that enhance the growth of certain strains of bacteria in the colon. Probiotics are thought to suppress inflammation in the gut, reduce impaired permeability of the intestines (see “Leaky Gut,” below) or reduce visceral hypersensitivity by balancing the composition of bacteria in the intestines. They may lead to improvement of symptoms of IBS. In one study, the use of the probiotic “Bifidobacterium infantis” improved global IBS symptoms by more than 20%. Another study showed that after a four week-treatment of IBS patients with “Lactobacillus acidophilus,” another probiotic found in yogurt, abdominal pain and discomfort were reduced by more than 20%. However, in another recent randomized, double-blind, placebo-controlled trial, in which IBS patients received a probiotic mixture of Lactobacillus paracasei ssp paracasei F19, Lactobacillus acidophilus La5 and Bifidobacterium Bb12 over six months, no differences in GI symptoms were noticed. There are a number of conflicting studies regarding the benefits of use of probiotics though they do appear to be well tolerated.
Leaky Gut
When this integrity is compromised, the permeability of the gut is altered which allows substances to penetrate the lining of the gut and enter the blood stream, a condition referred to as “leaky gut.” The “inappropriate” entry of these substances is thought to possibly trigger the immune system in ways that contribute to the symptoms of IBS, Crohn’s and Ulcerative Colitis as well as many psychiatric conditions.
The healthy balance of microorganisms in the gut is related to many factors, including diet. This is an emerging field of study with far more questions than answers. There is early evidence for the role of prebiotics and probiotics in the management of visceral pain syndromes but it is still too early to make definitive recommendations based on current research.
See “Leaky Gut.”
References
Pancreatitis Pain – Overviews
- visceral-sensation-pain-2009
- Alcoholic Pancreatitis – Pathogenesis, Incidence and Treatment with Special Reference to the Associated Pain – 2009
- The pain of chronic pancreatitis – a persistent clinical challenge – 2013
- Understanding and treatment of chronic pancreatitis – 2013
- Pharmacological pain management in chronic pancreatitis – 2013
- Pain in chronic pancreatitis – Managing beyond the pancreatic duct – 2013
- Pain sensation in pancreatic diseases is not uniform – The different facets of pancreatic pain – 2014
- Road map for pain management in pancreatic cancer – A review – 2016
- Towards a neurobiological understanding of pain in chronic pancreatitis – mechanisms and implications for treatment – 2017
- Pathogenesis and Treatment of Pancreatic Cancer Related Pain – 2020
- Chronic pancreatitis – review and update of etiology, risk factors, and management – 2018
- Managing Chronic Pancreatitis – Beyond Opioids – 2019
- Practical guide to the management of chronic pancreatitis – 2019
- Pathogenesis and Treatment of Pancreatic Cancer Related Pain – 2020
Pancreatitis Pain – Antioxidants
- Dietary antioxidants and chronic pancreatitis. – 1986
- Combined antioxidant therapy reduces pain and improves quality of life in chronic pancreatitis – 2006
- A randomized controlled trial of antioxidant supplementation for pain relief in patients with chronic pancreatitis – 2009
- Quality of life assessment in patients with chronic pancreatitis receiving antioxidant therapy – 2010
- Antioxidant therapy does not reduce pain in patients with chronic pancreatitis- the ANTICIPATE study – 2012
- Antioxidants and chronic pancreatitis- theory of oxidative stress and trials of antioxidant therapy – 2012
- Antioxidant Therapy for Pain Relief in Patients with Chronic Pancreatitis – Systematic Review and Meta-analysis – 2013
- Effect of antioxidant supplementation on surrogate markers of fibrosis in chronic pancreatitis- a randomized, placebo-controlled trial – 2013
- CYP3A-involving metabolism – 2014
- Antioxidants for pain in chronic pancreatitis. The Cochrane database of systematic reviews – 2014
- The effect of piperine on midazolam plasma concentration in healthy volunteers, a research on the
- Antioxidant therapy for patients with chronic pancreatitis- A systematic review and meta-analysis – 2015
- Role of methionine containing antioxidant combination in the management of pain in chronic pancreatitis- a systematic review and meta-analysis – 2015
- Antioxidant therapy in acute, chronic and post-endoscopic retrograde cholangiopancreatography pancreatitis – An updated systematic review and meta-analysis – 2015
- Attenuation of Morphine Withdrawal Syndrome by Various Dosages of Curcumin in Comparison with Clonidine in Mouse – Possible Mechanism – 2015
- Curcumin, Inflammation, and Chronic Diseases – How Are They Linked? – 2015
- Antioxidant therapy for pain reduction in patients with chronic pancreatitis- a systematic
review and meta-analysis – 2015 - Effect of curcuminoids on oxidative stress – A systematic review and meta-analysis of randomized controlled trials – 2015
- The Analgesic Effect of the Mitochondria-Targeted Antioxidant SkQ1 in Pancreatic Inflammation – 2016
- Ameliorating effect of antioxidants and pregabalin combination in pain recurrence after ductal clearance in chronic pancreatitis- Results of a randomized, double blind, placebo-controlled trial – 2016
- Coenzyme Q10 inhibits the activation of pancreatic stellate cells through PI3K:AKT:mTOR signaling pathway – 2017
- Curcumin, the golden nutraceutical – multitargeting for multiple chronic diseases – 2017
- Piperine ameliorates the severity of fibrosis via inhibition of TGF-β:SMAD signaling in a mouse model of chronic pancreatitis – 2019
- The Potential of Flavonoids for the Treatment of Neurodegenerative Diseases – 2019
- Antioxidant therapy in chronic pancreatitis—promises and pitfalls – 2019
- Enhanced Water Dispersibility of Curcumin Encapsulated in Alginate-polysorbate 80 Nano Particles and Bioavailability in Healthy Human Volunteers – 2019
- Pharmacokinetics, pharmacodynamics and PKPD modeling of curcumin in regulating antioxidant and epigenetic gene expression in human healthy volunteers – 2019
- Coenzyme Q10 Ameliorates Pancreatic Fibrosis via the ROS-Triggered mTOR Signaling Pathway – 2019
- Liposomal Encapsulated Curcumin Effectively Attenuates Neuroinflammatory and Reactive Astrogliosis Reactions in Glia Cells and Organotypic Brain Slices – 2020
- The Use of Curcumin as a Complementary Therapy in Ulcerative Colitis – A Systematic Review of Randomized Controlled Clinical Trials – 2020
- Selective phytochemicals targeting pancreatic stellate cells as new anti-fibrotic agents for chronic pancreatitis and pancreatic cancer – 2020
- Current Evidence to Propose Different Food Supplements for Weight Loss – A Comprehensive Review – 2020
- Obstacles against the Marketing of Curcumin as a Drug – 2020
- Nanocurcumin – A Promising Candidate for Therapeutic Applications. – 2020
- Dietary Patterns and Interventions to Alleviate Chronic Pain – 2020
Pancreatitis Pain – Antioxidants: CoQ10
- Coenzyme Q10 inhibits the activation of pancreatic stellate cells through PI3K:AKT:mTOR signaling pathway – 2017
- Coenzyme Q10 Ameliorates Pancreatic Fibrosis via the ROS-Triggered mTOR Signaling Pathway – 2019
Pancreatitis Pain – Antioxidants: Curcumin
- Clonidine in Mouse – Possible Mechanism – 2015
- Curcumin, Inflammation, and Chronic Diseases – How Are They Linked? – 2015
- Effect of curcuminoids on oxidative stress – A systematic review and meta-analysis of randomized controlled trials – 2015
- Curcumin, the golden nutraceutical – multitargeting for multiple chronic diseases – 2017
- Enhanced Water Dispersibility of Curcumin Encapsulated in Alginate-polysorbate 80 Nano Particles and Bioavailability in Healthy Human Volunteers – 2019
- Pharmacokinetics, pharmacodynamics and PKPD modeling of curcumin in regulating antioxidant and epigenetic gene expression in human healthy v
olunteers – 2019 - Liposomal Encapsulated Curcumin Effectively Attenuates Neuroinflammatory and Reactive Astrogliosis Reactions in Glia Cells and Organotypic Brain Slices – 2020
- The Use of Curcumin as a Complementary Therapy in Ulcerative Colitis – A Systematic Review of Randomized Controlled Clinical Trials – 2020
- Selective phytochemicals targeting pancreatic stellate cells as new anti-fibrotic agents for chronic pancreatitis and pancreatic cancer – 2020
- Obstacles against the Marketing of Curcumin as a Drug – 2020
- Nanocurcumin – A Promising Candidate for Therapeutic Applications. 2020
Pancreatitis Pain – Cannabinoids
Pancreatitis Pain – Central Sensitization
Pancreatitis Pain – Gabapentinoids (Gabapentin and Lyrica)
- pregabalin-reduces-pain-in-patients-with-chronic-pancreatitis-in-a-randomized-controlled-trial-2011
- effects-of-pregabalin-on-central-sensitization-in-patients-with-chronic-pancreatitis-in-a-randomized-controlled-trial-2012
- Ameliorating effect of antioxidants and pregabalin combination in pain recurrence after ductal clearance in chronic pancreatitis- Results of a randomized, double blind, placebo-controlled trial – 2016
- Pregabalin for decreasing pancreatic pain in chronic pancreatitis. – PubMed – NCBI
Pancreatitis Pain – Gut Microbiome
- Recent Advances on Nutrition in Treatment of Acute Pancreatitis – 2017
- The gut microbiota as a key regulator of visceral pain – 1017.pdf
- Gut Microbiota-Immune System Crosstalk and Pancreatic Disorders – 2018
- A Retrospective Study of Probiotic Use in Patients With Chronic Pancreatitis – 2019
- Man and the Microbiome- A New Theory of Everything? – PubMed 2019
- Disentangling What We Know About Microbes and Mental Health – 2019
- The Evolving Role of Gut Microbiota in the Management of Irritable Bowel Syndrome – An Overview of the Current Knowledge – 2020
- Gut microbiota regulates neuropathic pain – potential mechanisms and therapeutic strategy – 2020
- Stress and the Microbiota–Gut–Brain Axis in Visceral Pain – Relevance to Irritable Bowel Syndrome – 2015
- Visceral pain – gut microbiota, a new hope? – 2019
- The Role of the Gastrointestinal Microbiota in Visceral Pain – PubMed 2017
Pancreatitis Pain – Interventional Treatment
Pancreatitis Pain – Mechanisms of Pain
- Analgesia from a peripherally active kappa-opioid receptor agonist in patients with chronic pancreatitis – 2003
- Pancreatic neuropathy and neuropathic pain–a comprehensive pathomorphological study of 546 cases – 2009
- Pain mechanisms in chronic pancreatitis – of a master and his fire – 2011
- Unraveling the mystery of pain in chronic pancreatitis – 2012
- Perineural Mast Cells Are Specifically Enriched in Pancreatic Neuritis and Neuropathic Pain in Pancreatic Cancer and Chronic Pancreatitis – 2013
- Pain sensation in pancreatic diseases is not uniform – The different facets of pancreatic pain – 2014
- Pain and chronic pancreatitis – A complex interplay of multiple mechanisms – 2013
- Current understanding of the neuropathophysiology of pain in chronic pancreatitis – 2015
- Systematic mechanism-orientated approach to chronic pancreatitis pain – 2015
- The Analgesic Effect of the Mitochondria-Targeted Antioxidant SkQ1 in Pancreatic Inflammation – 2016
- Towards a neurobiological understanding of pain in chronic pancreatitis – mechanisms and implications for treatment – 2017
- Targeting nNOS ameliorates the severe neuropathic pain due to chronic pancreatitis – 2019
Pancreatitis Pain – Opioids
- Analgesia from a peripherally active kappa-opioid receptor agonist in patients with chronic pancreatitis – 2003
- Analgesia from a peripherally active kappa-opioid receptor agonist in patients with chronic pancreatitis – 2003
- Opioids for acute pancreatitis pain Cochrane Review – 2013
- The application of buprenorphine in acute and chronic pancreatitis – 2013
- Toward an effective peripheral visceral analgesic – responding to the national opioid crisis – 2018
- Opioid use for acute pancreatitis – Toward a research agenda to optimize patient safety – 2019
- Managing Chronic Pancreatitis – Beyond Opioids – 2019
Pancreatitis Pain, Opioids – Tapentadol (Nucynta)
- Patient considerations in the use of tapentadol for moderate to severe pain – 2013
- Opioid Safety and Concomitant Benzodiazepine Use in End-Stage Renal Disease Patients – 2019
- The mu-opioid receptor agonist:noradrenaline reuptake inhibition (MOR-NRI) concept in analgesia- the case of tapentadol – 2014
- Pharmacological rationale for tapentadol therapy – a review of new evidence
- First evaluation of tapentadol oral solution for the treatment of moderate to severe acute pain in children aged 6 to <18 – 2019
- Tapentadol vs oxycodone:naloxone in the management of pain after total hip arthroplasty in the fast track setting – an observational study – 2019
- Neural Circuits: An investigation into the noradrenergic and serotonergic contributions of diffuse noxious inhibitory controls in a
monoiodoacetate model of osteoarthritis – 2019 - Tapentadol Prolonged Release – A Review in Pain Management – 2018
- A combination pharmacotherapy of tapentadol and pregabalin to tackle centrally driven osteoarthritis pain – 2019
- Current considerations for the treatment of severe chronic pain- the potential for tapentadol – 2012
- Patient and Disease Characteristics Associate With Sensory Testing Results in Chronic Pancreatitis – 2019
- Efficacy and Safety of Long-Term Administration of Tapentadol in Relieving Chronic Pancreatitis Pain – PubMed 2017
- Efficacy and Safety of Long-Term Administration of Tapentadol in Relieving Chronic Pancreatitis Pain – 2017
Pancreatitis – Pancreatic Enzyme Replacement Therapy (PERT)
Pancreatitis – Palmitoylethanolamide (PEA)
Pancreatitis – Surgical and Endoscopic Management
- Total pancreatectomy with islet cell transplantation vs intrathecal narcotic pump infusion for pain control in chronic pancreatitis – 2016
- Earlier surgery improves outcomes from painful chronic pancreatitis – 2018
- Controversies on the endoscopic and surgical management of pain in patients with chronic pancreatitis – pros and cons! – 2019
- Surgery in Chronic Pancreatitis – Indication, Timing and Procedures – 2019
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices
.