
“My religion is very simple. My religion is kindness.”
~ 14th Dalai Lama
Dry Mouth (Xerostomia)
Dry mouth, or xerostomia, can be defined as the subjective sensation of persistent oral dryness and may also include sensations of burning in the mouth, mucosa, or tongue. There are many causes of dry mouth, with appropriate treatment based on the underlying cause(s).
Key to Links:
Grey text – handout
Red text – another page on this website
Blue text – Journal publication
.
Dry Mouth (Xerostomia)
Dry mouth generally indicates reduced salivary flow (hyposalivation) which may be either structural or functional. Structural causes of dry mouth include Sjogren’s Syndrome, sarcoidosis, post-radiation therapy and possibly diabetes. However, structural factors tend to be in the minority, with functional factors the usual cause. Functional factors include dehydration, chronic anxiety and medications, both prescription and non-prescription. Medications are by far the most common cause of dry mouth, with more than 400 medications known to contribute to symptoms of dry mouth.
Saliva
Saliva not only lubricates food, but also promotes clear speech, maintains nonirritating pH levels in the mouth, prevents dehydration of the oral mucous membranes, maintains dental integrity, and helps initiate digestion. Patients with reduced saliva production may have increases in potentially harmful bacteria that can increase dental decay and oral yeast infections. Subjective symptoms of dry mouth do not become apparent until unstimulated salivary volume falls below 50 percent.
Symptoms associated with dry mouth
Symptoms of reduced saliva may also include difficulty chewing, swallowing, and talking. There may also be potential long-term consequences including hoarseness and increased risk for esophagitis and esophageal reflux (GERD). Normal saliva production and subsequent swallowing of the saliva provides a protective bathing function of the esophagus allowing for flushing-out of stomach acids that may reflux into the esophagus. In the presence of reduced saliva and washout, the esophagus is more susceptible to irritation and erosion of the esophageal lining leading to GERD.
.
Medical conditions related to dry mouth
Certain medical conditions place individuals at risk for dry mouth including fibromyalgia, diabetes and Sjrogen’s syndrome. Individuals exposed to radiation treatment in the neck or oral cavity are at high risk. Symptoms of dry mouth often lead to excessive fluid intake (“polydipsia”) which may suggest other conditions associated with excessive fluid intake. Psychiatric patients may develop the syndrome of “psychogenic polydipsia,” a clinical disorder characterized by compulsive water drinking with excessive fluid intake (polydipsia) and excessive urination (polyuria). Most commonly found with chronic schizophrenia, other mental illnesses associated with psychogenic polydipsia are affective disorders, psychosis with onset during childhood, mental retardation, personality disorders, and tension/anxiety. Studies have reported that it can affect from 6 to 20 % of psychiatric patients. The underlying cause of this syndrome is unclear, and multiple factors have been implicated.
Excessive fluid intake associated with extreme polydipsia can lead to dangerously low blood levels of sodium (hyponatremia) which can progress to “water intoxication,” characterized by symptoms of confusion, lethargy, and psychosis, and seizures or even death. Excessive water intake can lead to swelling of the kidneys (hydronephrosis) leading to abdominal or back pain and impaired kidney function.
Medication Risks
Many or most chronic pain and fibromyalgia patients treated with medications complain about dry mouth. Most opioids are associated with dry mouth as are muscle relaxers and sleep medications. Antidepressants, whether used in the treatment of pain, anxiety or depression, are strongly associated with dry mouth. The treatment of cervical dystonia with Botox, especially Type B more than Type A, can lead to dry mouth.
While not a complete list, the following medications are frequently associated with dry mouth:
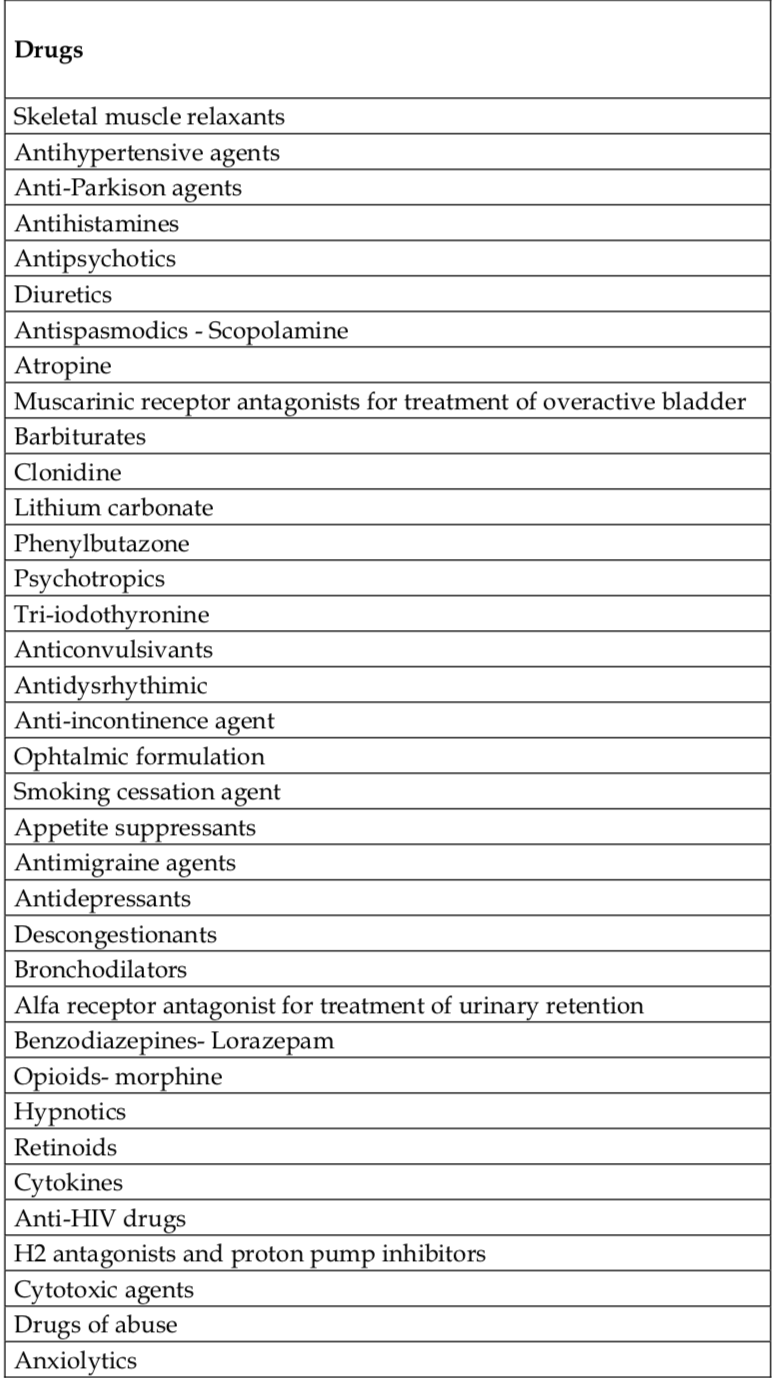
Medication / Dryness Severity Rating
Analgesics
Opioids / +
Antihistamines
Zantac (ranitidine) / +
Zyrtec (cetirizine) / +
Benadryl (diphenhydramine) / +++
Vistaril (hydroxyzine) / +++
Dramamine (dimenhydrinate) / +++
Antivert (meclizine) / +++
Anxiolytics
Benzodiazepines / +
Vistaril (hydroxyzine) / +++
Muscle Relaxers
Flexeril (cyclobenzaprine) / ++
Norflex (orphenadrine) / +++
Robaxin (methocarbamol) / +++
Tricyclic Antidepressants
Norpramin (desipramine) / +
Remeron (mirtazapine). / ++
Doxepin / +++
Elavil (amitriptyline) / +++
SNRI Antidepressants
Cymbalta (duloxetine) / 0
Effexor (venlafaxine) / 0
SSRI Antidepressants
Celexa (citalopram) / 0,+
Lexapro (escitalopram) / 0,+
Prozac (fluoxetine) / 0,+
Zoloft (sertraline) / 0,+
Paxil (paroxetine). / ++
Other Antidepressants
Trazadone / +
Wellbutrin (bupropion) / ++
Others
Phenergan (promethazine) / +++
Bentyl (dicyclomine) / +++
Seroquel (quetiapine) / +++
Ditropan (oxybutynin) / +++
Treatment Recommendations
Prescription Medications
Pilocarpine hydrochloride tablets, which increase salivary flow, have been found to improve dry mouth in patients with structural causes such as radiation-induced xerostomia and Sjogren’s syndrome. Pilocarpine may also be beneficial for the treatment of dry mouth associated with botulinum toxin type B.
Over-the-Counter products:
- Sodium fluoride
- Biotene
- Mucin-containing and xanthan gum
- Acid-tasting substances
- Acid-tasting substances
- Lemon pastilles
- Vitamin C tablets
- Sugar-free chewing gum & sweets
- Vegetables or fruits
References:
Dry Mouth and Medications – Overview
- Psychotropic Drugs – Implications for Dental Practice – 2008
- Medication-induced Xerostomia Secondary to Pain Management – 2011
- Antidepressants_side_effects_in_the_mouth
- Severity and Impact of Xerostomia in PatientsTreated with Botulinum Toxin Type B for Cervical Dystonia Observations on the Quality of Life of Patients with Xerostomia – 2014
- The use of oral pilocarpine in xerostomia and Sjögren’s syndrome. – PubMed – NCBI – 1999
Psychogenic Polydipsia
- Psychogenic Polydipsia – 2011
- Psychogenic Polydipsia – management challenges – 2017
- Psychogenic polydipsia review: etiology, differential, and treatment. – PubMed – NCBI – 2007
Dry Mouth Treatment
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices
.