
Griffonia (Griffonia simplicifolia), the main source of 5-HTP, is also known as African Black Bean.
L-tryptophan & 5-HTP (5-Hydroxytryptophan)
5-HTP (5-Hydroxy-L-tryptophan) is a substance that is made in the body from the amino acid, tryptophan, as an intermediate step in the body’s manufactuing of serotonin, an important neurtransmitter (brain chemical). 5-HTP is important and necessary for the production of serotonin and melatonin.
5-HTP is used in the treatment of depression, headaches, insomnia, fibromyalgia, obesity, carbohydrate craving, bulimia, narcolepsy and premenstrual syndrome.
The therapeutic use of neurotransmitter precursors (building blocks), such as amino acids L-tryptophan and 5-HTP, to facilitate the body’s production of neurotransmitters must take into account the balance that exists within the brain and nervous system between the many pathways and activities of multiple neurotransmitters. The healthy function of the brain and nervous system relies on a functional neurochemical balance and the disruption of this balance, either by a disease process or a treatment process, impairs healthy function.
Use of amino acid precursors, particularly long term, should therefore be engaged with caution and the guidance of a clinician well versed in this arena of therapeutics.
See Also:
- Complementary and Alternative Medications (CAM)
- Anxiety & Stress
- CAM Treatment – Depression
- CAM Treatment – Fibromyalgia
- CAM Treatment – Headaches
- Insomnia
.
L-tryptophan and 5-HTP
L-tryptophan in the Diet
L-tryptophan is one of the nine essential amino acid the body cannot manufacture and must be obtained through the diet. L-tryptophan is used to manufacture, among other molecules, serotonin and melatonin, two neurotransmitters necessary for healthy brain functioning.
Serotonin (5-hydroxy-tryptamine, 5-HT)
In the central nervous system, the neurotransmitter serotonin is known to regulate the main adaptive reactions and responses to environmental changes, such as mood-anxiety, sleep, cognition (thinking), nociception (pain perception), impulsivity, aggressiveness, libido, feeding behaviour, and body temperature.
In the peripheral nervous system and other parts of the body, serotonin modulates gut function, immune and inflammatory responses and the function of blood cells including platelets. Altered serotonin function is associated with mood-affective disorders including depression, autism and cognitive deficits, anorexia, bulimia nervosa and obesity, and other syndromes such as fibromyalgia, chronic fatigue syndrome, and irritable bowel syndrome (IBS).
L-tryptophan can be found in turkey, chicken, milk, potatoes, pumpkin, turnip and collard greens, seaweed, eggs, cheese, chocolate, oats, fish, poultry, spirulina, sesame, and sunflower seeds. The recommended dietary L-tryptophan daily intake for human adults ranges from 250 to 425 mg/day, corresponding to 3.5–6 mg/kg (mean 4 mg/kg) body weight per day Tryptophan is available as an over-the-counter dietary supplement. Because L-tryptophan is found in both animal and vegetable sources, a normal balanced diet generally assures enough L-tryptophan intake.
The typical Western diet contains approximately 500 mg of L-tryptophan per day but due to metabolism and competition with other amino acids, only 2–3% of L-tryptophan enters the brain where it is converted into 5-hydroxytryptophan (5-HTP) and then into serotonin. This competitve effect can be reduced by increasing the tryptophan ratio to other amino acids by supplementing with tryptophan.
While dietary deficiency is not usually a problem in developed countries, the regulation of L-tryptophan concentration in blood as well as its uptake to tissues and brain is the main variable related to health. The role of the gut microbiome is of growing interest as an aspect that is emerging as a link between nutrition, gut absorption, L-tryptophan regulation and health.
Dietary L-Tryptophan and Mood, Depression and Cognition (thought processing)
While our understanding of the neurochemistry of depression remains incomplete, one of the dominating neurobiological theories of depression is the monoamine hypothesis. The monoamine hypothesis of depression focuses on the imbalance of serotonin, dopamine and noradrenaline (the monamine neurotransmitters) as the mechanism of depression. The most frequently prescribed drugs in the treatment of mood disorders are selective serotonin reuptake inhibitors (SSRIs: Prozac, Paxil, Zoloft etc.) which enhance serotonin levels and serotonin and noradrenaline reuptake inhibitors (SNRIs: Cymbalta, Effexor, Savella) or tricyclic antidepressants (TCAs: Elavil, Doxepin, Despramine) which enhance serotonin and noradrenaline levels. To a limited extent these medications also increase dopamine levels.
Because side-effects are common with these drugs, a dietary approach to enhancing serotonin levels in the brain offers a safer approach. Because serotonin levels in the brain are dependent on the food-derived precursor tryptophan, foods rich in tryptophan such as chicken, soyabeans, cereals, tuna, nuts and bananas may serve as an alternative to improve mood and cognition.
Varying the amount of tryptophan in one’s diet has substantial effects on mood regulation and well-being, although research indicates that the relationship between tryptophan levels and mood is less straightforward than one might think (see Neurobiology of tryptophan below). While there are large individual differences in vulnerability to mood disorders, there are also large individual differences in responsiveness to antidepressant medications, as well as in responsiveness to serotonergic foods. One cross-national study revealed a negative correlation between dietary tryptophan and suicide rates.
Effects of acute tryptophan depletion on mood and cognitive functions in healthy subjects
When blood levels of tryptophan are depleted most women experienced a drop in their mood although this was not found in men. The reason for sex differences is not well understood but it is believed there are metabolic differences between men and women regarding serotonin production. The impact of tryptophan depletion is greater in people who are at greater risk for depression such as those with strong family history of depression o past history of depression.
Apart from mood, tryptophan depletion has been found to affect a number of cognitive functions in healthy individuals. Memory is significantly impaired as well as learning. As with mood, people who are at greater risk for depression are also at greater risk for more severe cognitive impairment.
Tryptophan Supplementation
From Food in the Stomach to Serotonin in the Brain
Tryptophan is one of many amino acids found in protein. When ingested, it is absorbed from the gastrointestinal tract into the bloodstream. When a meal containing protein is consumed a large proportion of tryptophan is metabolised in the liver, which does not happen with many other large neutral amino acids (LNAA). Thus the amount of tryptophan entering the circulation is much less compared with other LNAA, if the amounts of amino acids consumed are the same. However, the secretion of insulin in response to the intake of carbohydrates in the meal that in turn stimulates the uptake of LNAA into muscle tissue and reduces concentrations of all LNAA in the blood except tryptophan, which binds to albumin (a protein carrier in the blood) and circulates throughout the body.
Whether a meal increases the ratio of blood tryptophan levels compared with the blood levels of other LNAA (the TRP:LNAA ratio) depends on the amount of protein digested and the release of insulin. When tryptophan in the circulation reaches the brain capillaries it is transported across the blood – brain barrier. Here tryptophan has to compete with other LNAA for active transport into the brain. Therefore, not the blood level of tryptophan alone, but the TRP:LNAA ratio determines its rate of transport across the blood – brain barrier into the brain. Once inside the brain, tryptophan is taken up by the raphe nuclei and and is converted into serotonin.
Consequently, a protein-rich low-carbohydrate diet results in a decreased amount of tryptophan in the brain since the TRP:LNAA ratio in most protein is very low. Therefore, a protein-rich low-carbohydrate diet results in more competition for the transport system over the blood – brain barrier and consequently less transport of tryptophan into the brain.
Whereas consumption of a high-protein low-carbohydrate diet lowers tryptophan levels, consumption of a diet high in carbohydrates increases the Trp:LNNA ratio in blood and the brain (see neurobiology of tryptophan below). Combined with a low intake of protein, the plasma TRP:LNAA ratio shifts in favor of tryptophan and therefore increases the transport of tryptophan through the blood – brain barrier. This, however, only mildly elevates tryptophan levels in the brain, rarely exceeding an elevation of 25 % over baseline. Furthermore, most typical diets high in carbohydrates are high in protein as well, negating their effect on blood tryptophan levels.
Direct oral supplementation with tryptophan has been shown to raise blood and brain levels of serotonin. One study evaluated supplementing with a drink with a high tryptophan/LNAA ratio improved mood and cognition. However, studies suggest that there is an inverted U-shaped curve response for plasma tryptophan levels, with low and very high tryptophan levels impairing cognition, and moderate to high tryptophan levels improving cognition. This relationship is found for both healthy and vulnerable subjects.
Whereas this relationship may also exist for mood, the inverted U-shaped curve for plasma tryptophan levels and mood may be based on different tryptophan concentrations in healthy vs. vulnerable individuals. Further studies are emerging which may allow further understanding of effects and the mode of action of food-derived serotonergic components on mood, cognition and mechanisms.
To Summarize:
Studies indicate that those people with depression or at risk for depression are likely to experience a mood benefit from a short term tryptophan-rich diet with high Trp:LNAA ratios based on selected foods or tryptophan supplements. However, if taken to extremes excessive tryptophan intake can have the reverse effect of impairing mood.
Similarly, cognitive improvement in terms of memory and learning may be expected from a short term tryptophan-rich diet with high Trp:LNAA ratios based on selected foods or tryptophan supplements. However, if taken to extremes excessive tryptophan intake can have the reverse effect of impairing memory and learning.
L-Tryptophan Supplements
Supplementing with L-tryptophan has a long history of successful use. In one study of “normal” women, a tryptophan-rich drink lifted the mood and improved the stamina of normal women performing cognitive and emotional tests.
L-tryptophan has shown effectiveness as a sole agent in the treatment of depression. L-tryptophan has also been successfully and safely added to other anti-depressants, including fluoxetine (Prozac), clomipramine and lithium. The addition of tryptophan to fluoxetine in one study was associated with a greater improvement within the first week of treatment but not thereafter. There were no cases of serious toxicity of the combination; it was very well tolerated overall.
Dosing
In managing depression, a 1 gram dose of L- tryptophan is appreciably superior to 0.5 gram. Some authors advise potentially higher dose, up to 2-3 grams.
Safety
On its own, tryptophan is generally safe with mild side effects that include gastrointestinal side effects as well as headache, lightheadedness, drowsiness, dry mouth, visual blurring, muscle weakness, and sexual problems. In addition, there may be drug interaction with other agents such as antidepressants, that may lead to serotonin syndrome (See below, under 5-HTP). Tryptophan might act synergistically with other sedatives to cause over-sedation.
L-Tryptophan vs 5-hydroxytryptophan (5-HTP)
L-tryptophan which requires a transport molecule to enter the central nervous system, one that is also used by other amino acids. This situation leads to the potential for competition between amino acids for the transport molecule, leading to a limitation of how much L-tryptophan is transported. This has implications for the dietary intake of L-tryptophan where the presence of other amino acids affects L-tryptophan transport.
Compared with L-tryptophan which requires a transport molecule to enter the central nervous system, 5-HTP does not, so it crosses the blood brain barrier more readily and may have better effectiveness as a result. The use of 5-HTP may also offer the advantage of bypassing the conversion of L-tryptophan into 5-HTP by the enzyme tryptophan hydroxylase, which is the rate-limiting step in the synthesis of serotonin. Tryptophan hydroxylase can be inhibited by numerous factors, including stress, insulin resistance, vitamin B6 deficiency, and insufficient magnesium. In addition, these same factors can increase the conversion of L-tryptophan to kynurenine via tryptophan 2,3-dioxygenase, making less L-tryptophan available for serotonin production.
5-hydroxytryptophan (5-HTP)
5-hydroxytryptophan (5-HTP) is a chemical that the body makes from L-tryptophan. After tryptophan is converted into 5-HTP, it is then changed into serotonin. 5-HTP dietary supplements help raise serotonin levels in the brain. Serotonin helps regulate mood and behavior, and 5-HTP may be helpful with sleep, mood, anxiety, appetite, and pain sensation.
5-HTP is isolated from a natural source – a seed from an African plant (Griffonia simplicifolia). As a natural supplement, it is commonly used to treat a wide variety of conditions related to low serotonin levels, including the following, but there is limited evidence for its effectiveness.
Clinical Applications
Emerging research suggests dietary approaches are worth pursuing in supporting mental health as well various pain conditions. 5-HTP has a growing body of research to support it’s use in a variety of conditions.
5-HTP – Anxiety & Panic Disorder
While a number of natural substances have been reported to reduce anxiety, including Skullcap (genus Scutellaria), hops (Humulus lupulus), lemon balm (Melissa officinalis) and Valerian (Valeriana officinalis) root, tryptophan and 5-HTP are commonly used to promote relaxation and reduce anxiety. Ccompared to placebo, 5-HTP provides a moderate reduction multiple symptoms associated with anxiety.
.
Depression
Some studies suggest that 5-HTP may work as well as common anti-depressant medications for treating people with mild-to-moderate depression, including the class of selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine (Prozac), paroxetine (Paxil), citaloprm (Celexa), sertraline (Zoloft) and others. Studies have compared the effects of 5-HTP to SSRIs and found that 5-HTP was equally effective with fewer side effects. A 2012 study showed the antidepressant effect was evidentt within 2 weeks of treatment and was apparent in mild, moderate and severe depression. The therapeutic effectiveness of l-5-HTP was considered as equal to that of fluoxetine.
The overall strength of research with L-tryptophan and 5-HTP remains weak: more and larger studies are needed. However, 5-HTP has mostly been determined to be safe and effective and could be considered a first-line option for depression prior to starting prescription anti-depressants that are more likely to be accompanied by side effects.
Fibromyalgia
Studies have suggested that 5-HTP can improve multiple symptoms of fibromyalgia, including pain, anxiety, morning stiffness, and fatigue.
Headaches
Studies are spares, but 5-HTP has been roported to be effective for migraine and tension headaches, as well as chronic daily headaches which are often a combination of the two. Use of 5-HTP has been shown in limited studies to reduce the frequency and, especially, the severity and duration of headaches in s many as 71% of test subjects.
Insomnia
The effects of L-tryptophan on sleep have been investigated since the 1970s with varying support for its role in treating sleep disorders. Night time use has been shown to increase concentrations of both serotonin and melatonin; its proposed mechanism of action is thought to be through either melatonin enhancement or serotonergic effects.
In an experimental tryptophan depletion study, tryptophan depletion had a negative impact on sleep continuity, increasing stage 1 sleep and decreasing stage 2 sleep. There is growing evidence of an association between gut microbiota composition (gut microbiome) and sleep quality. A 2024 study concluded that 5-HTP supplementation can increase blood levels of serotonin and improve sleep quality in older adults and this benefit was best observed in poor sleepers. 5-HTP was also able to improve the gut microbiota composition in poor sleepers.
A number of studies demonstrate reduced sleep latency (time needed to fall asleep) while increased sleepiness during the day have been reported as side effects. Varying doses have been shown to significantly reduce sleep latency and increase subjective ratings of sleepiness in subjects with insomnia. A systematic review of sixty-four randomized controlled trials exploring the use of L-tryptophan to treat insomnia found mixed evidence. Studies suggest that 5-HTP allows more sound sleep and quicker onset of sleep compared with placebo.
Doses
Doses as high as 200 – 400 mg at night were required and up to 6 – 12 weeks to be fully effective.
5-HTP: Safety
Side effects of 5-HTP are generally mild and may include drowsiness, nausea, heartburn and gas. At very high doses, it is possible to precipitate serotonin syndrome, a potentially dangerous condition caused by too much serotonin. While serotonin syndrome resulting from combining 5-HTP with other medications is ‘‘rare,’’ it should be watched for especially if 5-HTP is taken with medications known to raises serotonin including opioids, anti-depressants and some muscle relaxers:
Serotonin Syndrome
Anti-depressants
SSRIs: Citalopram (Celexa), escitalopram (Lexapro), fluvoxamine (Luvox), paroxetine (Paxil), fluoxetine (Prozac), sertraline (Zoloft)
Tricyclics: Amitriptyline (Elavil), nortryptyline (Pamelor), imipramine (Tofranil)
Monoamine oxidase inhibitors (MAOIs): Phenelzine, (Nardil), tranylcypromine (Parnate) Nefazodone (Serzone)
Muscle Relaxers
Cyclobenzaprine (flereril)
Triptans (used to treat migraines)
Sumatriptan (Imitrex). Naratriptan (Amerge), Rizatriptan (Maxalt), Zolmitriptan (Zomig)
Other Prescription Medications
Amphetamines (Adderall), Dextromethorphan (Robitussin DM, Delsym)
Herbs and Supplements
Taking 5-HTP with other herbs and supplements that increase serotonin might lead to too much serotonin. Other herbs and supplements that increase serotonin levels include Hawaiian baby woodrose, L-tryptophan, S-adenosylmethionine (SAMe), and St. John’s wort.
See Serotonin Syndrome
Serotonin Withdrawal
Because our brains are homeostatic, meaning they function to maintain balance, when one supplements with 5-HTP for an extended period of time, the brain will adjust to this. While not commonly reported, it is possible that if the supplementation with 5-HTP is suddenly stopped or dramatically reduced, withdrawal symptome may occur. Some users report dizziness for several days after stopping 5-HTP while thers report a poor mood or fatigue for up to one week after they stop using 5-HTP.
Contaminants During Manufacturing
In 1989, a contaminant called Peak X was found in tryptophan supplements. Peak X was also found in some 5-HTP supplements, and there had been a few reports of EMS associated with taking 5-HTP. Researchers believed that an outbreak of eosinophilic myalgia syndrome (EMS, a potentially fatal disorder that affects the skin, blood, muscles, and organs) could be traced to the contaminated tryptophan, and the U.S. Food and Drug Administration pulled all tryptophan supplements off the market. However, the level of Peak X in 5-HTP was not high enough to cause any symptoms, unless very high doses of 5-HTP were taken.
The contaminant was found to occur as part of the manufacturing process and the products were reintroduced after clearance by the FDA, 5-HTP resourced from the plant, Griffonia simplicifolia, apparently has never been identified as causing EMS.
Since this time, 5-HTP has been under vigilance by consumers, industry, academia, and government for its safety. With the possible exception of one unresolved case of a Canadian woman, no definitive cases of toxicity have emerged despite the worldwide usage of 5-HTP for the last 20 years. Neither toxic contaminants similar to those associated with L-tryptophan, nor the presence of any other significant impurities have been detected in several sources of 5-HTP.
Recently, microbial engineering allows the production of 5-HTP from alternative biosynthetic routes, allowing better controlling of the presence of contaminants.
Dosing
Pediatric
5-HTP should not be given to children.
Pregnancy:
5-HTP should not be taken during pregnancy
.
Adult
Health care professionals generally recommend an initial dose of 50 mg of 5-HTP taken 1 – 3 times per day. but 5-HTP has been studied safely in higher doses for up to one year. In the multiple studies reviewed assessing 5-HTP for depression, the dose of 5-HTP ranged from 200 to 3,000 mg/day, more often from 200 to 300 mg/day, with dose scheduling ranging twice- to 4-times-per-day. The recommended dosing frequency was 3-times-per-day in a recent review article.
5-HTP: Neurobiology
As an essential amino acid, L-tryptophan is a metabolically complex nutrient that is incorporated in many diiferent pathways to maintain health. Only 10% of L-tryptophan is generally directed into the pathways resuting in production of serotonin and melatonin, while 90% of L-tryptophan conversion is directed into another pathway to kynurenine via tryptophan 2,3-dioxygenase, making L-tryptophan unavailable for serotonin production.
Both supplements of L-tryptophan and 5-HTP have been used in treatment, but the use of 5-HTP may offer the advantage of bypassing the conversion of L-tryptophan into 5-HTP by the enzyme tryptophan hydroxylase, which is the rate-limiting step in the synthesis of serotonin. Tryptophan hydroxylase can be inhibited by numerous factors, including stress, insulin resistance, vitamin B6 deficiency, and insufficient magnesium. In addition, these same factors can increase the conversion of L-tryptophan to kynurenine.
Monamine Transporter Optimization (MTO)
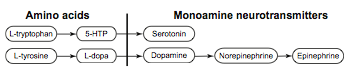
While depression may be due to serotonin dysfunction, depression may also be related to other neurotransmitter dysfunction, such as dopamine, norepinephrine and/or epinephrine, the catecholamine type neurotransmitters.
The synthesis, metabolism, and transport of serotonin and dopamine, along with their amino acid precursors, are primarily controlled by the functional status of transporters. Serotonin, dopamine, and their amino acid precursors must be transported across cell walls. Transporters dominate, control and regulate the manufacture and breakdown of neurotransmitters. Because 5-HTP does not require transporters to cross from the blood into the brain, supplementing with 5-HTP alone can lead to increased and unbalanced levels of serotonin which can result in competitive inhibition of the transport of dopamine and its precursors thereby compromising and depleting dopamine levels.
Supplementing with 5-HTP alone, or in an unbalanced manner, can also result in depletion of the other catecholamines, norepinephrine and epinephrine, negatively affecting theses neurotransmitter-related disease processes. When deficient catecholamine neurotransmitter levels contribute to depression, supplementing with 5-HTP alone may be contraindicated since it may further deplete dopamine and norepinephrine, thereby worsening the depression. This contraindication is not limited to depression, but extends to all other disease processes in which dysfunction of a catecholamine component is involved, including attention-deficit hyperactivity disorder (ADHD), seasonal affective disorder, obesity, and generalized anxiety disorder.
References:
Tryptophan – Overviews
Tryptophan – Dietary
- Food can lift mood by affecting mood-regulating neurocircuits via a serotonergic mechanism. 2014 – PubMed – NCBI
- Food-derived serotonergic modulators – effects on mood and cognition – 2013
- Conversion L-tryptophan to melatonin in the gastrointestinal tract – 2012
- Effect of orally administered L-tryptophan on serotonin, melatonin, and the innate immune response in the rat. – PubMed – NCBI
- Acute tryptophan depletion in humans – a review of theoretical, practical and ethical aspects – 2013
Tryptophan – Depression
- Comparison of the antidepressant action of tryptophan, tryptophan:5-hydroxytryptophan combination and nomifensine. 1984 – PubMed – NCBI
- L-Tryptophan as an antidepressive agent in the management of treatment-resistant unipolar depression in borderline personality disorder – 2015
- Tryptophan and 5-Hydroxytryptophan for depression (Review) – 2002
5-HTP – Overviews
- 5-HTP: MedlinePlus Supplements
- 5-Hydroxytryptophan – A Clinically-Effective Serotonin Precursor – 1998
- 5-HTP efficacy and contraindications – 2012
- 5-Hydroxytryptophan (5-HTP)- Natural Occurrence, Analysis, Biosynthesis, Biotechnology, Physiology and Toxicology – 2020
5-HTP – Alcohol Witdrawal Syndrome
5-HTP – Anxiety & Panic Disorder
- Effect of a serotonin precursor and uptake inhibitor in anxiety disorders; a double-blind comparison of 5-hydroxytryptophan, clomipramine and placebo. 1987 – PubMed – NCBI
- Behavioral, neuroendocrine, and biochemical effects of 5-hydroxytryptophan administration in panic disorder.1990 – PubMed – NCBI
- Formulations of dietary supplements and herbal extracts for relaxation and anxiolytic action: Relarian. 2009 – PubMed – NCBI
- Conversion L-tryptophan to melatonin in the gastrointestinal tract – 2012
- Effect of orally administered L-tryptophan on serotonin, melatonin, and the innate immune response in the rat. – PubMed – NCBI
- Tryptophan and 5-hydroxytryptophan for depression.2001 – PubMed – NCBI
5-HTP– Depression
- CAM Therapies to Promote Healthy Moods – 2007 5-HTP efficacy and contraindications – 2012
- Depression vulnerability and 5-hydroxytryptophan prophylaxis.1980 – PubMed – NCBI
- Chemoprophylaxis of depressions. An attempt to compare lithium with 5-hydroxytryptophan.1981 – PubMed – NCBI
- In search of the mode of action of antidepressants: 5-HTP:tyrosine mixtures in depression. 1984- PubMed – NCBI
- Comparison of the antidepressant action of tryptophan, tryptophan:5-hydroxytryptophan combination and nomifensine. 1984 – PubMed – NCBI
- Treatment strategy in depression. II. MAO inhibitors in depression resistant to cyclic antidepressants: two controlled crossover studies with trany… 1988 – PubMed – NCBI
- L-5-hydroxytryptophan alone and in combination with a peripheral decarboxylase inhibitor in the treatment of depression. 1988 – PubMed – NCBI
- Essential elements in depression and anxiety_PartI – 2014
- Tryptophan and 5-Hydroxytryptophan for depression (Review) – 2002
- Comparative study of efficacy of l-5-hydroxytryptophan and fluoxetine in patients presenting with first depressive episode. 2013 – PubMed – NCBI
- Clinical depression: an evidence-based integrative complementary medicine treatment model.2011 – PubMed – NCBISecond-tier natural antidepressants – Review and critique – 2010
- Tryptophan and 5-hydroxytryptophan for depression.2001 – PubMed – NCBI
- 5-Hydroxytryptophan: a review of its antidepressant efficacy and adverse effects. 198- PubMed – NCBI
- Essential elements in depression and anxiety_PartI – 2014
- Food can lift mood by affecting mood-regulating neurocircuits via a serotonergic mechanism. 2014 – PubMed – NCBI
- Increased plasma levels of competing amino acids, rather than lowered plasma tryptophan levels, are associated with a non-response to treatment in major depression – 2016
- Second-tier natural antidepressants – Review and critique – 2010
5-HTP – Fibromyalgia
- Primary fibromyalgia syndrome and 5-hydroxy-L-tryptophan: a 90-day open study. – PubMed – NCBI
- Double-blind study of 5-hydroxytryptophan versus placebo in the treatment of primary fibromyalgia syndrome. – PubMed – NCBI
5-HTP – Headaches
- A double-blind, placebo-controlled investigation of the effects of Passiflora incarnata (passionflower) herbal tea on subjective sleep quality. – PubMed – NCBI
- L-5HTP treatment in primary headaches: an attempt at clinical identification of responsive patients. – PubMed – NCBI
- [Treatment of essential headache in developmental age with L-5-HTP (cross over double-blind study versus placebo)]. 1984 – PubMed – NCBI
- 5-Hydroxytryptophan versus methysergide in the prophylaxis of migraine. Randomized clinical trial. 1986 – PubMed – NCBI
- Serotonin precursors in chronic primary headache. A double-blind cross-over study with L-5-hydroxytryptophan vs. placebo.1985 – PubMed – NCBI
- [Comparison of the effect of 5-hydroxytryptophan and propranolol in the interval treatment of migraine]. 1991 – PubMed – NCBI
- L-5-Hydroxytryptophan in the prophylaxis of chronic tension-type headache: a double-blind, randomized, placebo-controlled study.. 2000. – PubMed – NCBI
5-HTP – Insomnia & Sleep
- Effects of 5-hydroxytryptophan on fragmentation of REM sleep in alcoholics. 1975 – PubMed – NCBI
- A randomized, placebo-controlled trial of an amino acid preparation on timing and quality of sleep. 2010- PubMed – NCBI
- Oral nonprescription treatment for insomnia: an evaluation of products with limited evidence.2005 – PubMed – NCBI
- Updates on Nutraceutical Sleep Therapeutics and Investigational Research – 2015
- Gut microbiota and sleep- Interaction mechanisms and therapeutic prospects – 2024
- The impact of 5-hydroxytryptophan supplementation on sleep quality and gut microbiota composition in older adults_ A randomized controlled trial – PubMed – 2024
5-HTP – Menopausal Symptoms
- Gabapentin for the treatment of hot flashes in women with natural or tamoxifen-induced menopause: a systematic review and meta-analysis – PubMed Health
- Treatment of Menopausal Hot Flashes with 5-Hydroxytryptophan – 2009
5-HTP – Microbiome
- Gut microbiota and sleep- Interaction mechanisms and therapeutic prospects – 2024
- The impact of 5-hydroxytryptophan supplementation on sleep quality and gut microbiota composition in older adults_ A randomized controlled trial – PubMed – 2024
5-HTP – Obesity
- The effects of oral 5-hydroxytryptophan administration on feeding behavior in obese adult female subjects.1989 – PubMed – NCBI
- Satiety and amino-acid profile in overweight women after a new treatment using a natural plant extract sublingual spray formulation. 2009 – PubMed – NCBI
- Eating behavior and adherence to dietary prescriptions in obese adult subjects treated with 5-hydroxytryptophan. 1992- PubMed – NCBI
5-HTP– Obsessive -Compulsive Disorder (OCD)
5-HTP – Neurobiology
.
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices
.