“For there was never yet a philosopher that could endure the toothache patiently.”
– William Shakespeare
Dental Pain
Toothaches most often arise from an irritated nerve in a tooth, but there are many other sources of dental pain. Other causes include dental infection, gum disease, plaque, dental decay (caries), cracked teeth and broken or cracked fillings or crowns. Also, there are conditions where pain originates from outside the mouth but radiates to the mouth, thus giving the wrong impression that the pain is of dental origin. This commonly occurs with problems in the jaw joint (temporomandibular joint or TMJ), ears or sinuses and even from the heart, as a manifestation of a heart attack.
Managing dental pain effectively begins with identifying the source of the pain. There are some simple steps one can take to narrow down the possible cause and identify a possible effective treatment.
See also:
See also:
Integrative, Complimentary and Alternative Medicine (CAM)
CAM – Dental Pain:
Key to Links:
- Grey text – handout
- Red text – another page on this website
- Blue text – Journal publication
Dental Pain – Diagnosis
The character and pattern of oral pain can provide clues to the cause of the pain.
Intermittent, sharp, shooting pain
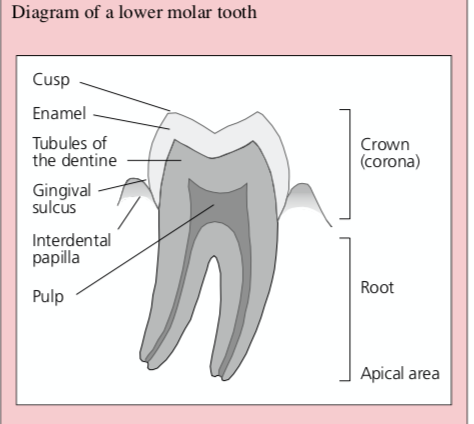
Intermittent, sharp, shooting pain can be generalized or confined to one area in the mouth but likely represents pain arising from a dental nerve. Dental nerve pain is often triggered by exposure to hot, cold or sweets. It may be due to damage to the external surface of the tooth, the enamel, due to tooth decay with cavity formation (caries), a loose or cracked filling, or a cracked or broken tooth which exposes the underlying layer of dentine. Dental nerve pain may also occur with exposure of dentine from gum recession due to gum disease. When pain is triggered by chewing or biting down on a tooth and the pain tends to be localised to that affected tooth., it suggests a cracked tooth or a cracked or loose filling.
Particularly severe pain that can be intermittent, sharp or shooting and perceived as facial or dental in origin can also come from irritation of the trigeminal nerve, a major nerve of the face. This condition is called trigeminal neuralgia. It is episodic, occurs in clusters of events and may be triggered by a soft touch to the face or even wind blowing against the face.
Dull, throbbing, persistent pain
Generalized Pain
Generalized dental sensitivity occurs when the gums recede from the tooth (gingival recession) due to chronic gum disease (gingivitis), or there has been a recent scaling procedure by the dentist during teeth cleaning. This sensitivity may also occur with general tooth wear due to a high acid diet or gastric reflux (GERD).
Localized Pain
The most common dental cause of localized dull, throbbing persistent pain is caries which is often recurrent. A fractured dental cusp involving the inner components of the tooth (the pulp) may also be associated with this type of pain. When caries is severe and progressive, destruction of the tooth may follow with possible development of a dental abscess (periapical infection). In this case the tooth may be tender to percussion (tapping on the tooth) and there may be significant swelling of the face. In severe cases, the infection may spread to the face as a cellulitis and may be accompanied by fever.
There is a great deal of variation in how the pain from dental decay (caries) is experienced by different patients, but it commonly starts as a sharp stabbing pain that becomes progressively dull and throbbing. At first the pain may be caused by a stimulus such as heat, cold or biting, but it then becomes spontaneous and remains for a considerable time after removal of the stimulus. The pain may radiate and be referred to other areas of the mouth. It may cause the person to have difficulty sleeping and may be worsened by lying down. Applying warm compresses tend to make the pain worse whereas cold compresses tend to relieve it. Initially, the pain may be intermittent with no regular pattern over months or even years. If a periapical infection develops, patients may no longer complain of pain in response to a thermal stimulus, but rather of sensitivity on biting.
Dental Treatment
Individual Conditions
Dental Sensitivity
For tooth sensitivity the use of a desensitising toothpaste and a reduction of acid in the diet will help improve the symptoms. Using a fluoride mouth-rinse may also help.
Dental Caries
In the case of caries, a lost filling or fractured tooth, there is disruption of the protective coating of enamel which exposes the underlying layer of dentine which contains nerves that become irritated and sources of pain. If possible, covering the area of disrupted enamel will protect the exposed nerve and reduce pain. Dentists can apply a covering coat of glass ionomer cement (GIC) or zinc oxide eugenol (ZOE) to provide a temporary patch but these materials are not available to the consumer.
Dental Abscess
An abscessed tooth is a dental condition in which the nerve of the tooth, also referred to as the dental pulp, has become infected. The infection usually occurs when a dental cavity (tooth decay) goes untreated and spreads deep within the tooth. The greater the amount of decay, the closer it gets to the dental nerve, and the more likely the nerve can become compromised. The infection can also occur from a broken or cracked tooth where the dental pulp is exposed to the oral environment. The bacteria that cause an abscess can spread down the length of the roots and into the surrounding bone. An infection can also occur between the gums and root of the tooth, called a periodontal abscess.
Treatment of dental abscess generally requires either root canal treatment or tooth removal. In cases associated with cellulitis or fever, representing possible rapid spread of bacteria, there may be a surgical emergency. Antibiotics are likely to be required but antibiotic treatment alone is not adequate as drainage of the infection is necessary to resolve the problem. The antibiotic of choice should cover gram positive and anaerobic bacteria such as a penicillin or cephalexin (Keflex), clindamycin or metroniazole (Flagyl).
Avulsed or Broken Tooth
It is essential to reimplant permanent teeth as soon as possible. The tooth that is out of the socket and/or broken fragments should be stored in a physiological medium such as normal saline or milk. Before reimplantation, the root surface should be cleaned gently to remove debris and the root should not be touched with the fingers. Avulsed deciduous (baby) teeth are generally not reimplanted, as they may become fused to the alveolar bone and impede subsequent emergence of the permanent tooth.
Treating Dental Pain
Antibiotics
While antibiotics are appropriate in the management of certain dental infections, they are not indicated if the pain results from inflammatory (non-infectious) or neuropathic mechanisms. The severity of pain is not a reliable determination of acute infection. Antibiotics should be limited to patients with signs of infection such as fever or lymph node involvement, cellulitis, spreading infection, or a rapid onset of severe infection.
When antibiotics are indicated for managing a dental infection, an antibiotic effective against aerobic and anaerobic gram-positive cocci is generally recommended. As such, penicillin (PenVK) or amoxicillin are often prescribed as generally effective and inexpensive. Another antibiotic option is clindamycin which is useful in the management of infections caused by aerobic and anaerobic Gram-positive cocci. Recent research has found that clindamycin appears to have pharmacological potential beyond its antibiotic properties.
Clindamycin has been found to have benefits for reducing inflammation by suppressing production of pro-inflammatory mediators. Additionally, clindamycin may reduce both acute and chronic pain by activation of opioidergic mechanisms. Altogether, these results suggest that clindamycin may be a preferred choice for dental infections associated with inflammation and pain.
Over-the Counter Products
NSAIDS (Non-Steroid Anti-inflammatory Drugs) & Acetaminophen (Tylenol)
Over-the-counter (OTC) NSAIDs such as ibuprofen (Advil) or naproxen (Aleve) are generally considered the most effective, first drug of choice in managing dental pain for those who tolerate NSAIDs. NSAIDs inhibit the synthesis of prostaglandins that are the inflammatory molecules that trigger pain. They are often more effective than opioids, which are only considered when OTC treatments are ineffective. There does not appear to be any evidence that one NSAID is more effective than another for dental pain in general, athough individuals may experience preferences.
While NSAIDs alone may often be sufficient to provide adequate pain relief, the addition of acetaminophen (Tylenol) will enhance the benefit from NSAIDs and reduce the need for opioids. Currently there are over-the-counter products that combine these two agents in one pill.
CBD (Cannabidiol) for Acute Dental Pain
A 2024 study, the first randomized clinical trial testing CBD for managing emergency dental pain, evaluated 40 patients with acute dental pain with a single dose of either 10mg/kg or 20mg/kg dose of CBD. (This is equivalent to 4.5 mg/lb 0r 9 mg/lb). )It was demonstrated that both doses provided the same, significant pain relief within 3 hours. The higher dose providing a more rapid onset of relief than the lower dose (15 min vs 30 min) and a more rapid onset of 50% relief ( (60 min vs 120 min). The lower dose was associated with calmness, relaxation, or sleepiness) wheras the higher dose was also more likely to experience diarrhea and abdominal pain which resolved in the same day.
When comparing CBD with other commonly used analgesics for acute dental pain including ibuprofen, ibuprofen with acetaminophen, and oxycodone-10mg with acetaminophen, CBD provided similar benefits. Using the comparator of NNTs, namely the number of patients needing treatment before 1 patient experiences a minimum of 50% pain relief, the NNT for CBD-10 was 3.1 and CBD-20 was 2.4 compared to ibuprofent 400-600mg (2.5-2.7) ibuprofen 200mg/acetaminophen 650mg (1.6) and oxycodone-10/acetaminophen 650mg (2.3).
This study showed for the first time that CBD only can provide more than 70% analgesia to patients with emergency dental pain while maintaining a safe drug profile with minimal side effects.
“Chasing pain” vs. Pre-emptive Pain Control
“Chasing pain,” that is, waiting for the local anesthetic to wear off and then start taking pain medicine when the pain intensity reaches a moderate to severe level, is not the best way to control pain after dental procedures. Studies have demonstrated that pre-surgical ibuprofen 400 mg significantly delays the onset of postoperative pain compared to a Percocet 10 mg. The rationale behind this approach is to reach therapeutic blood levels of the NSAID before the surgical trauma generates prostaglandins. NSAIDs inhibit prostaglandin synthesis only, they do not reduce the response to prostaglandins once they have been formed.
Optimal Strategy
It is recommended to pre-emptively use a combination of ibuprofen 200 mg or 400 mg with acetaminophen 500 mg or 1,000 mg, respectively, either an hour before surgery or immediately after surgery before local anesthesia wears off. Afterwards, continue around-the-clock dosing for up to 3 days.
Eugenol
A number of commercial products contain eugenol, the active ingredient in cloves, including “Red Cross Toothache Medication.” Eugenol is applied topically to the tooth or gums and helps numb the pain (See Cloves below).
Home Remedies
There are lot of home remedies recommended for use in dental pain. Unfortunately, there is little scientific research to support or refute these claims. The following list is provided only for consideration of use with no confirmed evidence of benefit. They do, however, appear to be safe.
Salt Water Rinses
A salt water rinse nay be an effective first-line treatment. As a natural disinfectant, salt water rinsing can help loosen food particles and debris that may be stuck in between the teeth and may help reduce inflammation. To prepare a salt water rinse, mix 1/2 teaspoon of salt into a glass of warm water and swish it as a mouthwash.
Hydrogen Peroxide Rinses
A hydrogen peroxide rinse may also help to relieve pain and inflammation. In addition to killing bacteria, hydrogen peroxide can reduce plaque and heal bleeding gums. Make sure to properly dilute the hydrogen peroxide. To do this, mix 3 percent hydrogen peroxide with equal parts water and use it as a mouthwash. Don’t swallow it.
Cold Compress
Applying a cold compress to the area of dental pain causes the blood vessels in the area to constrict, slows nerve conduction and makes pain less severe. The cold can also reduce swelling and inflammation. To apply a cold compress, hold a towel-wrapped bag of ice to the affected area for 20 minutes at a time and repeat every few hours as needed.
Cloves & Clove oil

Cloves contain eugenol, a natural antiseptic, and have been used to treat toothaches for centuries because the oil in cloves can effectively numb pain and reduce inflammation. Whole cloves can be found in grocery stores and clove is also available in capsule or powder form. The most effective approach for dental pain is to use clove oil, available at most drugstores.
One may dab a small amount of clove oil onto a cotton ball and apply it to the affected area or rub a tiny amount of clove oil on the gums. It is recommended to dilute the clove oil with a few drops of a carrier oil, such as olive oil, because too much undiluted clove oil may irritate the gums. Treatment can be applied a few times per day.
People with bleeding disorders or who are taking blood-thinning medication should be careful when using clove products because they can increase the risk of abnormal bleeding.
Garlic
Garlic contains a chemical called allicin, which acts as a natural antibiotic and may help fight a dental infection. To apply, crush a garlic clove to create a paste and apply it to the affected area. Alternatively, one can slowly chew a clove of fresh garlic.
Vanilla Extract
Vanilla extract may help to numb pain: dab a small amount of vanilla extract onto a cotton ball and apply it directly to the affected area a few times per day.
Peppermint Tea Bags
Peppermint tea bags can be used to numb pain and soothe sensitive gums. To use, allow a used tea bag to cool down then apply it to the affected area. It should still be slightly warm.
Guava Leaves
Guava leaves may have anti-inflammatory properties and antimicrobial activity that can help heal wounds and aid in oral care. To use, chew on fresh guava leaves or add crushed guava leaves to boiling water to make a mouthwash.
Wheatgrass
Wheatgrass is believed by some to have healing properties, relieve inflammation in the mouth and prevent infection. Its high chlorophyll content may also fight bacteria. To use wheatgrass, simply use wheatgrass juice as a mouthwash.
Thyme
Thyme has antibacterial and antioxidant properties that may help to treat toothaches. After diluting thyme essential oil with water, add a few drops onto a cotton ball and apply it to the affected area. Alternatively, one can also add thyme essential oil to a small glass of water and use as a mouthwash.
Opioids
The most opioids most commonly prescribed for dental pain are: oxycodone, hydrocodone, codeine, and tramadol, with 85% of oral surgeons responding that they “almost always” prescribed opioids following 3rd molar extractions. While recent research suggests that opioids may possess a peripheral anti-inflammatory effect that is distinct from how NSAIDs work, as single entities (not combined with acetaminophen or ibuprofen), opioids perform miserably in the control of postsurgical dental impaction pain. Studies show that 5 mg oxycodone is no more effective than an over-the-counter (OTC) dose of acetaminophen 500 mg (Tylenol) or no better than placebo. A 60 mg dose of codeine is inferior to aspirin 650 mg for dental pain, and tramadol (100 mg) is only slightly more effective than placebo. Even an oral dose of 60 mg immediate-release morphine is inferior to ibuprofen 400 mg.
CGRP Agents
Recently a new class of drugs that interact with the calcitonin gene receptor protein (CGRP), an important player in the pain pathways related to migraine headaches, have been introduced for treating migraine headaches. Rimegepant (Nurtec), a CGRP blocker, has recently beeen approved for both aborting and preventing migraine headaches and due the role of CGRP in dental pain it may offer benefit for acute or chronic dental or orofacial pain.
See:
Dental Pain – Overview
- Management of acute dental pain – a practical approach for primary health care providers – 2001
- Multimodal management of dental pain with focus on alternative medicine: A novel herbal dental gel 2016
- Understanding and managing dental and orofacial pain in general practice – 2016
Dental Pain – New Articles
- CGRP Induces Differential Regulation of Cytokines from Satellite Glial Cells in Trigeminal Ganglia and Orofacial Nociception – 2019
- A double-blind randomized crossover study to evaluate the timing of pregabalin for third molar surgery under local anesthesia – PubMed
- Pregabalin in patients with postoperative dental pain – PubMed
- Ion Channels Involved in Tooth Pain – 2019
- Ion Channels of Nociception – 2020
- Is There a Relationship between Throbbing Pain and Arterial Pulsations? – 2012
- Understanding and managing dental and orofacial pain in general practice – 2016
- Efficacy and safety of combined piroxicam, dexamethasone, orphenadrine, and cyanocobalamin treatment in mandibular molar surgery – 2006
- Nonsteroidal Anti-Inflammatory Drugs and Opioids in Postsurgical Dental Pain – 2020
- Clindamycin inhibits nociceptive response by reducing tumor necrosis factor-α and CXCL-1 production and activating opioidergic mechanisms – PubMed. – 2020
Dental Pain – Eugenol
- Effectiveness of 0.2% chlorhexidine gel and a eugenol-based paste on postoperative alveolar osteitis in patients having third molars extracted: a r… – PubMed – NCBI
- Eugenol Inhibits Calcium Currents in Dental Afferent Neurons – 2005
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices