
“We never see ourselves as others see us.”
– Oliver Hardy
Reward Deficiency Syndrome (RDS)
Reward Deficiency Syndrome (RDS) is the common denominator underlying both chemical and behavioral addictions but it also contributes to compulsive disorders such a obsessive compulsive disorder (OCD) as well as eating disorders, PTSD, ADD and certain anger disorders. It also overlaps with and influences chronic pain.
“Reward Deficiency Syndrome,” a term first coined by Ken Blum in 1995, can be defined as:
“A brain reward genetic dissatisfaction or impairment that results in aberrant pleasure seeking behavior that includes drugs, excessive food, sex, gaming/gambling and other behaviors.”
These other behaviors include an array of disorders, such as PTSD, ADHD, Tics, Tourette Syndrome, autism, Asperger Syndrome, OCD, “compulsive” sexual practices, binge eating and others. The relationships of these disorders becomes apparent with the understanding of the common genetic factors underlying them. RDS afflicts approximately one-third of the people in America.
See:
Reward Deficiency Syndrome (RDS)
Reward Deficiency Syndrome (RDS) & Addiction
Reward Deficiency Syndrome (RDS) & Chronic Pain
Genetic Testing: Reward Deficiency Syndrome
Genetic Testing: Individual DNA Alleles
See also:
Definitions and Terms Related to Pain
Key to Links:
Grey text – handout
Red text – another page on this website
Blue text – Journal publication
.
Reward Deficiency Syndrome (RDS)
“Reward Deficiency Syndrome” (RDS) is a genetically based condition known to afflict approximately one-third of people in America.
Happiness and Reward
All humans have an innate, primary drive to be happy and feel good. Feeling good is based largely on achieving a sense of reward in one’s life and at the same time a lack of serious stress. Humans, and animals, are reward-driven creatures. Behavior is largely driven by the reward experienced as a result of that behavior. The feel good of satiety is the reward of eating, driven by hunger. Social acceptance and the feeling of being loved is a powerful reward underlying the strong drive for social and human interaction. Experiencing the climax of the sexual act is another powerful reward driving human behavior.
The primary rewarding effects of behaviors (and substances) occur in several brain structures that link basic emotions and connect them to memories, which drive behavior. These behaviors produce sensations of pleasure in response to actions that support survival (e.g., eating, sex) but also sensations of fear in response to potential dangers. These sensations in turn trigger the endocrine (hormone) and autonomic nervous systems, stimulating bodily responses. The brain’s reward and stress systems are interactive and reinforce life-sustaining behaviors.
The neurochemical and neuroanatomic correlates of feeling good and maintaining a sense of well-being are based in the reward system of the brain. While the specifics of this reward system are explored further below, it is sufficient to understand that achieving this “holy grail” of feeling good is the result of a cascade of neurochemical events leading to the maintenance of adequate levels of the neurotransmitter dopamine in the brain’s reward center, the nucleus accumbens (NAc).
Any disruption in this brain reward cascade can lead to insufficient levels of dopamine in the NAc which is associated with an impaired sense of well-being and a condition of “reward deficiency.” There are both many factors that can contribute to reward deficiency and many ways in which reward deficiency may manifest.
Factors contributing to a reward deficiency state may be genetic, environmental or experiential. Genetic factors are inheritable, including genes made up of DNA that may be passed from generation to generation. In addition, there are epigenetic factors as well, in which specific conditions can turn genes on or off, thereby determining whether the genetic trait is manifest or not. Epigenetic factors are environmentally or experientially modifiable but they can also be passed from generation to generation.
While genetic and epigenetic factors are likely to be targeted as methods of treatment in the near future, they are not tools generally available at this time. Therefore, environmental and experiential factors that contribute to reward deficiency are probably the most important in the sense that they are variables that can be addressed and modified.
Environmental factors that impact the reward system include exposure to drugs, alcohol, food and nutrition. The common denominator of all addictive drugs is their capacity to spike dopamine levels in the reward system, especially the NAc. This capacity of these drugs coupled with an underlying state of reward deficiency is what predisposes certain individuals to substance or behavioral addictions.
See: Reward Deficiency Syndrome (RDS) & Addiction
Experiential factors include social interactive experiences, sleep and stress, as well as behaviors that enhance or reduce these factors. Chronic pain is a powerful experiential factor that contributes to disruption in the reward system.
See: Reward Deficiency Syndrome (RDS) & Chronic Pain
The Reward Deficiency Syndrome (RDS)
The reward system, located in the midbrain and centered in the nucleus accumbens (NAc) engages several neurotransmitters including dopamine, serotonin, GABA and norepinephrine. The most prominent of these neurotransmitters, dopamine, functions largely in the experience of pleasure (reward) and the reduction of stress. The basis of the “Reward Deficiency Syndrome (RDS)” is the condition of sub-optimal dopamine levels in the NAc and related brain areas.
Individuals with inadequate levels of dopamine in the reward center (NAc) due to genetic, environmental or experiential circumstances, experience an exaggerated “feel-good” response to substances (drugs) and behaviors that increase their inadequate dopamine levels. This heightened response leads to a powerful, rewarding drive to re-experience the effects of the substance or behavior. A variety of activities are known to increase dopamine levels, including behaviors such as sex, binge eating, gambling, thrill-seeking, computer gaming and even expressing strong anger. The dopamine drive inherent in these behaviors is believed to contribute to their addictive potential, especially in those people who may have genetic, environmental or experiential conditions that predispose them to chronic low dopamine levels.
In addition to substance and non-substance addictive behaviors, reward deficiency is also thought to be an underlying contributor to impulsive, obsessive-compulsive disorders and certain personality disorders as well as other conditions, including PTSD (see below).

Evaluating Risk for Reward Deficiency Syndrome (RDS)
Environmental Risks
Vulnerability to RDS differs from person to person and is influenced by environmental factors including social environment, peer pressure, levels of stress, diet and nutrition, availability of drugs and their method of administration.
Experiential Risks
The individual’s experiences also dictate risk for RDS. These experiences include physical, emotional and sexual abuse which may in turn also lead to PTSD. A persons capacity and skill with adapting to stress is an important variable. Sleep deprivation and impaired quality of sleep also impact a person’s vulnerability to RDS. Chronic pain and inadequacy of pain management contribute to significant vulnerability.
Genetic Risks
A persons family history of RDS-associated conditions provides clues to their genetic risk of developing RDS. This has been well demonstrated with alcoholism and other drug addictions. Family history is also a risk factor for ADD/ADHD and other behavioral disorders. Researchers estimate that genetic and epigenetic factors account for between 40% to 60% of a person’s vulnerability to addiction, especially alcoholism. Genetic testing for risk of RDS is now available with a simple oral swab for saliva. The results of genetic testing can be informative regarding prevention and management of many RDS-associated conditions.
See: Genetic Testing: Reward Deficiency Syndrome (RDS)
Translational Risks
It is also important to point out that sometimes treatment of an RDS-associated condition such as addiction may cause the underlying RDS to manifest as another RDS-associated condition. For example, management of opioid addiction with abstinence often triggers addictive eating behaviors and craving for sweets. It has also been demonstrated that patients with eating disorders who undergo gastric sleeve surgery experience increased risk for gambling and other behavioral disorders after surgery. The basis for this translational risk lies in the fact that the underlying dopamine deficiency is not addressed by abstinence from an addictive drug or behavior. This continued dopamine deficiency fuels the drive for dopamine enhancement through other substances or behaviors and, of course, the drive to relapse into the original addiction.
Management of Reward Deficiency Syndrome (RDS)
There is good evidence that supports “dopamine homeostasis” as a goal of treatment for RDS.
Genetic-based Approaches to Management of RDS
Understanding how genetic variants impact the reward system and dopamine levels provides opportunities for alternative approaches to treating addiction and other RDS-associated conditions. Through use of the GARS panel of genetic testing, individual DNA-based vulnerabilities impacting dopamine maintenance can be identified. Subsequently, dopamine balance can be accomplished through the use of genetically guided neuro-nutrients (including SynaptaGenX and other supplement variants). Restoring dopamine balance has been shown to be effective at reducing RDS symptoms and severity, especially in certain addictions and chronic pain conditions.
See:
Genetic Testing: Individual DNA Alleles
SynaptaGenX
Environment-based Approaches to Management of RDS
Environmental factors, especially chronic pain and stress, have a tremendous impact on the reward system and dopamine levels. Adequately treating pain, reducing stress and the manifestations of stress are important in the treatment of RDS. Mindful exercises including meditation, Tai Chi, yoga and deep relaxation techniques are useful modalities in managing stress and restore dopamine levels. Not to be overlooked, aerobic exercise reduces stress and positively impacts most RDS-associated conditions and is strongly recommended.
See: Using the Mind & Dopamine Enhancement
Dopamine-boosting dietary approaches designed to enhance dopamine have been proposed. The use of nutri-genomic supplements based on genetic testing are also advised, (see above).
See: Dopamine Diet & SynaptaGenX
Experiential Factors in Management of RDS
Memory plays a cornerstone role in many RDS-associated conditions and can be a major contributing influence in behaviors related to RDS. Hypnosis is a very useful tool that can be incorporated to effectively “re-write” memories and defuse their role in maladaptive behaviors and emotions.
See:
Using the Mind
Hypnosis
Dopamine Enhancement
The Neurobiology of the Reward System
Several areas of the brain are i
nvolved in the perception of reward, pleasure and well-being. The prefrontal cortex modifies pleasure and pain signals from other brain areas. Feelings of reward are focused in the core of the limbic system where neurons in the ventral tegmental area (VTA) release the neurotransmitter dopamine into the nucleus accumbens (NAc). Nerve activity within this VTA–NAc circuit is essential to experience reward, although other areas in the brain reward circuit also exert strong influences. For example, the hippocampus contributes memories relevant to an experience that modifies the reward experience positively or negatively. The amygdala adds important emotional information about a reward stimulus that contributes to the motivational impact of the experience. In addition, parts of the prefrontal cortex (i.e., anterior cingulate and orbito-frontal cortices) modify pleasure and pain signals to help integrate available information and allow the individual to decide whether to initiate or suppress a particular behavior in response to a stimulus.
See: Neurobiology of Pain
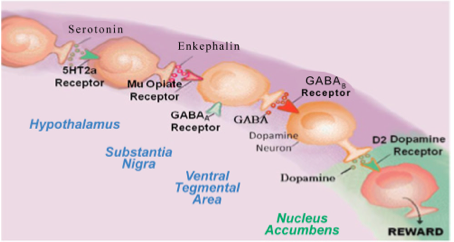
The brain reward cascade starts in the hypothalamus, located at the base of the midbrain area called the mesolimbic system where the neurotransmitter serotonin acts to activate the enkephalins (one type of brain endorphin); the enkephalins are released from the hypothalamus and stimulate mu-opioid receptors in another part of the brain called the substantia nigra. The substantia nigra contains the inhibitory neurotransmitter GABA that stimulates GABA-B receptors that projects to the ventral tegmental area (VTA) brain region where dopamine neurons are inhibited to allow for just the right amount of dopamine to be released at the nucleus accumbens (NAc) (the reward site of brain).
The Brain Reward Cascade
More About Dopamine
It is theorized that increased levels of dopamine were part of a general physiological adaptation related to survival around two million years ago by primitive human species and later (beginning approximately 80,000 years ago) further evolved as a result of dietary changes and other environmental and social factors. Species with high dopamine levels are thought to be characterized by higher intelligence, a sense of personal destiny, religious/cosmic preoccupation and an obsession with achieving goals and conquests. According to theory, dopaminergic drive is extremely goal-oriented, fast-paced, and even manic sometimes, given that dopamine is known to increase activity levels, speed up our internal clocks and create a preference for new experiences.
Dopamine is manufactured from L-tyrosine (a dietary amino acid found in meat) in several areas of the brain, especially in the nucleus accumbens (NAc), the center of reward experience. Activities, behaviors and chemicals or medications that contribute to higher dopamine levels in the NAc correlate with greater sensations of pleasure and well-being.
Dopamine is released in the mesolimbic reward pathways in the NAc and ventral tegmental area (VTA). The limbic system and medial prefrontal cortex process the reward value of a stimulus through the dynamic interplay between tonic and phasic dopamine levels.
Tonic dopamine levels are characterized by a slow, low-volume release of dopamine that is induced by glutamate and then degraded by the enzymes catechol-O-methyltransferase (COMT) and monamine oxidase (MAO). The tonic level of dopamine is a baseline measure of the amount of reward one generally experiences or expects from any given stimulus.
In contrast, phasic dopamine levels are characterized by an instant, high-volume release in response to a drug or pleasant stimulus but is quickly reduced by dopamine receptor (D2) feedback that inhibits further dopamine release and activates the dopamine reuptake transporter to remove excess dopamine from the extracellular space. Phasic levels of dopamine are determined by the difference between the received and expected value of a stimulus, and is the measure of the net value of reward for any particular stimulus. This net value is then processed by the limbic system and medial prefrontal cortex through which the incentive value and importance of the rewarding stimulus is summarized and committed to memory.
Dopamine functions as a neurotransmitter that activates 5 receptors in the brain, dopamine receptors D1 through D5. Research indicates that one receptor in particular, the D2 receptor, is of particular importance in achieving pleasure and reward. The relative abundance of D2 receptors in the NAc influences the capacity of dopamine to trigger pleasure and sustain a sense of well-being. The more D2 receptors an individual has, the greater capacity for reward the individual can experience. There are genetic (DNA) variants that determine whether an individual is born with a fewer or greater number of D2 receptors. Those who have fewer D2 receptors require more dopamine to achieve a sense of reward, pleasure and perception of well-being. Thus, there is a genetic influence, or drive, towards behaviors that increase dopamine levels, including ingestion of medications and chemicals that increase dopamine levels in the reward and pleasure center of the brain. Chemicals and drugs that are known to increase dopamine levels include sugar and the addictive drugs: cocaine, opioids, marijuana, alcohol, amphetamines, methamphetamines and others.
RDS – Overview
- The Addictive Brain – All Roads Lead to Dopamine – 2012
- Hatching the behavioral addiction egg – Reward Deficiency Solution System – 2014
- Sex, Drugs, and Rock ‘N’ Roll – Hypothesizing Common Mesolimbic Activation as a Function of Reward Gene Polymorphisms – 2012
- “Dopamine homeostasis” requires balanced polypharmacy – Issue with destructive, powerful dopamine agents to combat America’s drug epidemic
- Neurodynamics of relapse prevention-neuronutrient approach to outpatient DUI offenders
- Genetic Addiction Risk Testing Coupled with Pro Dopamine Homeostasis
- Pro-dopamine regulator, KB220Z, attenuates hoarding and shopping behavior in a female, diagnosed with SUD and ADHD
- Neuro-Nutrient Effects on Weight Loss in Carbohydrate Bingers – an open clinical trial
- Enkephalinase Inhibition – Regulation of Ethanol Intake in Genetically Predisposed Mice
- The D2 dopamine receptor gene as a determinant of reward deficiency syndrome – 1996
- Dopamine D2 receptor gene variants: association and linkage studies in impulsive-addictive-compulsive behaviour. – PubMed – NCBI
- Activation instead of blocking mesolimbic dopaminergic reward circuitry is a preferred modality in the long term treatment of reward deficiency syndrome (RDS) – a commentary – 2008
- Reward deficiency syndrome: a biogenetic model for the diagnosis and treatment of impulsive, addictive, and compulsive behaviors. – PubMed – NCBI
- Association of polymorphisms of dopamine D2 receptor (DRD2), and dopamine transporter (DAT1) genes with schizoid:avoidant behaviors (SAB). – PubMed – NCBI
- Reward deficiency syndrome: genetic aspects of behavioral disorders. – PubMed – NCBI
- The D2 dopamine receptor gene as a predictor of compulsive disease: Bayes’ theorem. – PubMed – NCBI
- Delayed P300 latency correlates with abnormal Test of Variables of Attention (TOVA) in adults and predicts early cognitive decline in a clinical se… – PubMed – NCBI
- Neurological correlates of brain reward circuitry linked to opioid use disorder (OUD) – Do homo sapiens acquire or have a reward deficiency syndrome? – 2020
RDS – ADD
- Attention-deficit-hyperactivity disorder and reward deficiency syndrome – 2008
- Reward Deficiency Syndrome – Attentional Arousal Subtypes, Limitations of Current Diagnostic Nosology, and Future Research – 2015
- Neurogenetic interactions and aberrant behavioral co-morbidity of attention deficit hyperactivity disorder (ADHD) -dispelling myths – 2005
- Epigenetics in Developmental Disorder – ADHD and Endophenotypes
- Low Dopamine Function in Attention Deficit:Hyperactivity Disorder – Should Genotyping Signify Early Diagnosis in Children? – 2014
- Enhancement of attention processing by Kantroll in healthy humans: a pilot study. – PubMed – NCBI
- Pro-dopamine regulator, KB220Z, attenuates hoarding and shopping behavior in a female, diagnosed with SUD and ADHD
RDS – Exercise
- Physical Exercise Interventions for Drug Addictive Disorders – 2017
- Basal ganglia dysfunction contributes to physical inactivity in obesity – 2017
- Running from Disease – Molecular Mechanisms Associating Dopamine and Leptin Signaling in the Brain with Physical Inactivity, Obesity, and Type 2 Diabetes – 2017
RDS – Gaming
</ span>
RDS – Genetics
- Multilocus Genetic Composite Reflecting Dopamine Signaling Capacity Predicts Reward Circuitry Responsivity 2012
- Genetic Addiction Risk Score (GARS) – Testing For Polygenetic Predisposition and Risk to Reward Deficiency Syndrome (RDS) – 2011
- Neurogenetic Impairments of Brain Reward Circuitry Links to Reward Deficiency Syndrome (RDS) – Potential Nutrigenomic Induced Dopaminergic Activation
RDS – Obesity
- Reward Deficiency Syndrome Studies of KB220 Variants
- Mood, food, and obesity
- Dopamine and glucose, obesity, and reward deficiency syndrome – 2014
- Dopamine for “wanting” and opioids for “liking”: a comparison of obese adults with and without binge eating. – PubMed – NCBI
- “Liking” and “Wanting” Linked to Reward Deficiency Syndrome (RDS) – Hypothesizing Differential Responsivity in Brain Reward Circuitry – 2012
- Neuro-Genetics of Reward Deficiency Syndrome (RDS) as the Root Cause of “Addiction Transfer”- 2011
- Physical Exercise Interventions for Drug Addictive Disorders – 2017
- Basal ganglia dysfunction contributes to physical inactivity in obesity – 2017
- Running from Disease – Molecular Mechanisms Associating Dopamine and Leptin Signaling in the Brain with Physical Inactivity, Obesity, and Type 2 Diabetes – 2017
- Incorporating food addiction into disordered eating – the disordered eating food addiction nutrition guide (DEFANG) – 2017
- Do Dopaminergic Impairments Underlie Physical Inactivity in People with Obesity? – 2016
- Pilot clinical observations between food and drug seeking derived from fifty cases attending an eating disorder clinic – 2016
- A meta-analysis of the relationship between brain dopamine receptors and obesity – a matter of changes in behavior rather than food addiction? – 2016
- Increasing dopamine D2 receptor expression in the adult nucleus accumbens enhances motivation – 2013
- Food restriction markedly increases dopamine D2 receptor (D2R) in a rat model of obesity as assessed with in-vivo muPET imaging ([11C] raclopride) … – PubMed – NCBI
- LOW DOPAMINE D2 RECEPTOR INCREASES VULNERABILITY TO OBESITY VIA REDUCED PHYSICAL ACTIVITY NOT INCREASED APPETITIVE MOTIVATION – 2016
- Dopamine and glucose, obesity, and reward deficiency syndrome – 2014
- Food Addiction, High-Glycemic-Index Carbohydrates, and Obesity. – PubMed – NCBI – 2018
- Association of dopamine D2 receptor and leptin receptor genes with clinically severe obesity. – PubMed – NCBI
- LG839: anti-obesity effects and polymorphic gene correlates of reward deficiency syndrome. – PubMed – NCBI
RDS –
Chronic Pain
- Hypothesizing that brain reward circuitry genes are genetic antecedents of pain sensitivity and critical diagnostic and pharmacogenomic – 2009
- A Multi-Locus Approach to Treating Fibromyalgia by Boosting Dopaminergic Activity in the Meso-Limbic System of the Brain – 2014
- Love as a Modulator of Pain – 2017
- Comorbidity of alcohol use disorder and chronic pain – Genetic influences on brain reward and stress systems – 2017
- Reward Circuitry Plasticity in Pain Perception and Modulation – 2017
- Modulation of pain, nociception, and analgesia by the brain reward center – 2016
- Pharmacology of enkephalinase inhibitors: animal and human studies. – PubMed – NCBI 198
- Analgesic properties of enkephalinase inhibitors: animal and human studies. – PubMed – NCBI 1985
- DL-phenylalanine markedly potentiates opiate analgesia – an example of nutrient:pharmaceutical up-regulation of the endogenous analgesia system. – PubMed – NCBI – 2000
- Iatrogenic opioid dependence is endemic and legal – Genetic addiction risk score (GARS) with electrotherapy a paradigm shift in pain treatment programs – 2013
- Mesolimbic dopamine signaling in acute and chronic pain – implications for motivation, analgesia, and addiction – 2016
- Microglia Disrupt Mesolimbic Reward Circuitry in Chronic Pain Positive emotions and brain reward circuits in chronic pain – 2016
- The indirect pathway of the nucleus accumbens shell amplifies neuropathic pain – 2016
- Dopamine and Pain Sensitivity – Neither Sulpiride nor Acute Phenylalanine and Tyrosine Depletion Have Effects on Thermal Pain Sensations in Healthy Volunteers – 2013
- Dopamine Precursor Depletion Influences Pain Affect Rather than Pain Sensation – 2014
- Insurance Companies Fighting the Peer Review Empire without any Validity – 2018
RDS – PTSD
- Neuro-psychopharmacogenetics and Neurological Antecedents of Posttraumatic Stress Disorder – Unlocking the Mysteries of Resilience and Vulnerability – 2010
- Diagnosis and Healing In Veterans Suspected of Suffering from Post-Traumatic Stress Disorder (PTSD) Using Reward Gene Testing and RewardCircuitry Natural Dopaminergic Activation-2012
- Putative dopamine agonist (KB220Z) attenuates lucid nightmares in PTSD patients – Role of enhanced brain reward functional connectivity and homeostasis redeeming joy – 2015
RDS – Sleep
RDS – Treatment
RDS Treatment – Overview
- Clinically Combating Reward Deficiency Syndrome (RDS) with Dopamine Agonist Therapy as a Paradigm Shift – Dopamine for Dinner? 2015
- Neurogenetics and Nutrigenomics of Neuro-Nutrient Therapy for Reward Deficiency Syndrome (RDS)
- A Novel Precision Approach to Overcome the “Addiction Pandemic” by Incorporating Genetic Addiction Risk Severity (GARS) and Dopamine Homeostasis Restoration – 2021
- Psychoactive Drugs Like Cannabis -Induce Hypodopaminergic Anhedonia and Neuropsychological Dysfunction in Humans – 2021
RDS Treatment – Meditation
RDS Treatment – Music Therapy
RDS Treatment – SynaptaGenX
SynaptaGenX – Overviews
SynaptaGenX – Buptrenorphine
SynaptaGenX – Fibromyalgia
SynaptaGenX – Lucid Nightmares
- Putative dopamine agonist (KB220Z) attenuates lucid nightmares in PTSD patients – Role of enhanced brain reward functional connectivity and homeostasis redeeming joy – 2015
- Using the Neuroadaptagen KB200zTM to Ameliorate Terrifying, Lucid Nightmares in RDS Patients – the Role of Enhanced, Brain- Reward, Functional Connectivity and Dopaminergic Homeostasis – 2015
SynaptaGenX – PTSD
- Putative dopamine agonist (KB220Z) attenuates lucid nightmares in PTSD patients – Role of enhanced brain reward functional connectivity and homeostasis redeeming joy – 2015
- Diagnosis and Healing In Veterans Suspected of Suffering from Post-Traumatic Stress Disorder (PTSD) Using Reward Gene Testing and RewardCircuitry Natural Dopaminergic Activation-2012
SynaptaGenX – Sleep
.
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
Supplements recommended by Dr. Ehlenberger may be purchased commercially online or at Accurate Clinic.
Please read about our statement regarding the sale of products recommended by Dr. Ehlenberger.
Accurate Supplement Prices
.