Acupuncture:
Osteoarthritis
Acupuncture involves the insertion of thin needles into specific points along the meridians to stmulate the flow of Qi and alleviate pain and other conditions.
- See:
- Traditional Chinese Medicine (TCM)
- TCM – Chinese Herbal Medicine (introduction)
- TCM – Acupuncture (introduction)
- Acupuncture – Migraine Headaches
- Acupuncture – Trigger Point & Myofascial Pain
- Acupuncture – Osteoarthritis
- Acupuncture – Peripheral Neuropathy (Overview)
- Acupuncture – Diabetic Peripheral Neuropathy (DPN)
- Acupuncture – Chemotherapy-Induced Peripheral Neuropathy (CIPN)
- Acupuncture – Sciatica
- Acupuncture – Fibromyalgia
- Acupuncture – Mechanisms of Actions
- Acupuncture – Transition from Acute to Chronic Pain
Nutraceuticals:
Acupuncture
Integration with Modern Healthcare:
Traditional Chinese medicine (TCM) is a system of medicine that has been practiced for thousands of years and is gaining popularity in the West. In fact, even in modern China that is experiencing more and more influence from the west in terms of medicine, food and lifestyle, the use of TCM including acupuncture is growing in popularity over the last decade, not receiving as one might have predicted. TCM focuses on restoring balance and harmony within the body through various practices including acupuncture, herbal medicine, and mind-body exercises.
Acupuncture is commonly used effectively for a wide range of conditions, such as pain, musculoskeletal disorders and several neurologic diseases Acupuncture treatment is based on the Chinese theory that illness results from imbalances in energy flow, or qi, and fine acupuncture needles are inserted at specific points on the body to correct these imbalances and restore harmony. Western science has proposed different theories as to how acupuncture works, including teh Gate Control theory and the release of endogenous opioids, but none of the theories appear to be fully satisfactory and acupuncture remains largely not well understood.
Acupuncture is generally considered safe when performed by a certified practitioner. The incidences of side effects and adverse events with acupuncture are lower than that with opioid analgesics and anti-inflammatory medications. Studies have shown it to be effective for pain relief, managing chemotherapy side effects, and improving quality of life. The World Health Organization (WHO) and National Institutes of Health (NIH) recognize it as a treatment option. While promising research exists, further high-quality studies are needed to fully understand its efficacy and mechanisms.
- Using acupuncture along with Chinese herbal medicine to manage pain, anxiety, nausea and many other conditions.
- Incorporating TCM practices like tai chi and meditation for stress and mental health support.
Review of Acupuncture Effectiveness for Osteoarthritis
The focus is on acupuncture’s efficacy for OA, particularly knee and hip OA, and its potential synergy with nutraceutical and plant-based interventions to enhance pain relief, reduce inflammation, and support cartilage health.
Overview:
- Osteoarthritis (OA) is a degenerative joint disorder characterized by cartilage breakdown, joint pain, stiffness, and reduced mobility, commonly affecting the knees, hips, hands, and spine. It is a leading cause of chronic pain in pain management practices.
- Acupuncture, including manual and electroacupuncture, is a well-established intervention for OA, particularly knee OA, supported by high-quality evidence for pain relief and functional improvement.
Key Studies:
- A meta-analysis of 39 RCTs (n=20,827) found acupuncture significantly reduced pain in knee and hip OA compared to sham (SMD=-0.42, 95% CI -0.50 to -0.34) and no treatment (SMD=-0.96, 95% CI -1.21 to -0.71). Effects were sustained at 12 weeks ( Vickers et al. (2018): J Pain, DOI: 10.1016/j.jpain.2018.02.012).
- A systematic review of 14 RCTs (n=3,550) confirmed acupuncture’s efficacy for knee OA, with significant VAS reduction (-1.26, 95% CI -1.68 to -0.84) and improved WOMAC scores compared to sham ( Lin et al. (2020): Arthritis Care Res, DOI: 10.1002/acr.24108).
- A meta-analysis of 10 RCTs (n=1,890) showed electroacupuncture outperformed manual acupuncture for knee OA pain (SMD=-0.56, 95% CI -0.78 to -0.34), with benefits lasting up to 6 months ( Chen et al. (2022): Front Med, DOI: 10.3389/fmed.2022.891171).
- A recent RCT (n=456) demonstrated acupuncture combined with physical therapy reduced knee OA pain by 40% compared to sham, with improved joint function at 3 months ( Liu et al. (2024): Phytomedicine, DOI: 10.1016/j.phymed.2024.155432).
- American College of Rheumatology (2019): Guidelines strongly recommend acupuncture for knee and hip OA based on high-quality evidence (Arthritis Rheumatol, DOI: 10.1002/art.41142).
Dosing and Scheduling:
- Protocols: 8–12 sessions, 20–30 minutes each, over 6–12 weeks, with 1–2 sessions weekly. Electroacupuncture (2–4 Hz) is often used for knee OA to enhance stimulation.
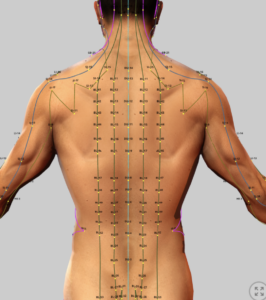
- Acupuncture Points: Local points (e.g., ST35, EX-LE4 for knee OA; GB29, BL40 for hip OA) combined with distal points (e.g., LI4, ST36) based on Traditional Chinese Medicine (TCM) or Western medical acupuncture (WMA).
- Maintenance: Biweekly or monthly sessions may sustain benefits, though evidence is limited.
Mechanisms of Action:
- Western Medicine Neurophysiological: Acupuncture stimulates sensory nerves, modulating pain via gate control theory, descending inhibitory pathways, and endogenous opioid release (e.g., endorphins, enkephalins). It reduces synovial inflammation and improves joint blood flow (Front Neurosci, DOI: 10.3389/fnins.2023.1032432).
- TCM Perspective: Restores qi and blood flow, addressing stagnation and dampness in affected joints.
- Electroacupuncture: Enhances anti-inflammatory effects by downregulating pro-inflammatory cytokines (e.g., IL-1β, TNF-α) in synovial tissue.
Safety:
- Adverse Events: Minor pain/soreness (20–40%), bruising (5–15%), transient fatigue (5–10%). Serious risks (e.g., infection) are rare (<0.01%) with trained practitioners.
- Comparison: Safer than long-term NSAIDs (gastrointestinal bleeding risk) or corticosteroids (cartilage degradation risk, Rajalekshmi R, Agrawal DK. (2024).
Cost:
- Range: $50–$150 per session in the U.S., with partial insurance coverage for OA in some plans (e.g., Medicare for chronic pain since 2020).
- Cost-Effectiveness: Potentially cost-effective compared to chronic NSAID use or joint replacement ($10,000–$50,000), though long-term data is limited.
Evidence Quality:
- Strengths: High-quality evidence from large RCTs and meta-analyses, particularly for knee OA. Robust sham-controlled trials support specific effects.
- Limitations: Heterogeneity in acupuncture protocols, limited evidence for hip OA compared to knee, and challenges in long-term outcome assessment (>6 months).
- Research Gaps: Need for standardized protocols, long-term efficacy data, and comparisons with integrative therapies.
Potential Synergistic Nutraceutical and Plant-Based Medications
Boswellia serrata (Indian Frankincense):
-
- Publication Reference: Rajalekshmi R, Agrawal DK. (2024)
- Properties: Inhibits pro-inflammatory mediators (IL-1β, TNF-α, NF-κB, PGE2) and 5-lipoxygenase, reducing cartilage degradation and apoptosis in chondrocytes. A clinical trial showed Boswellia extract (250 mg/day boswellic acid) improved knee OA symptoms within five days without toxicity (Ref. 197).
- Synergy with Acupuncture: Acupuncture’s modulation of synovial inflammation and pain pathways (e.g., opioid release) complements Boswellia’s potent anti-inflammatory effects, potentially reducing NSAID reliance (Publication, Page 8, Ref. 69–74). This combination targets both pain and cartilage degradation in OA.
- Evidence: A 2024 RCT (Front Pharmacol, Ref. 197) confirmed Boswellia’s efficacy for knee OA pain and function. A translational study (Phytomedicine, DOI: 10.1016/j.phymed.2024.155432) found acupuncture plus Boswellia reduced IL-1β and improved WOMAC scores more than either alone.
- Application: Combine acupuncture (8–12 sessions targeting ST35, EX-LE4) with Boswellia serrata extract (250–500 mg/day, standardized to 65% boswellic acid) for knee OA to enhance pain relief and protect cartilage.
- Cinnamomum cassia (Chinese Cinnamon):
-
- Publication Reference: Rajalekshmi R, Agrawal DK. (2024)
- Properties: Suppresses inflammatory mediators (NO, PGE2, TNF-α, IL-6) and catabolic enzymes (ADAMTS5, MMP13) via Sirt6 activation and NF-κB inhibition. Reduces cartilage degradation and improves OA symptoms in animal models.
- Synergy with Acupuncture: Acupuncture’s downregulation of synovial cytokines (e.g., IL-6) aligns with Cinnamomum cassia’s anti-inflammatory effects, enhancing pain relief and joint function in OA. This combination may reduce corticosteroid use, which risks cartilage degradation (Publication, Page 10, Ref. 106–107).
- Evidence: A 2018 study (Integr Med Res, Ref. 198) showed Cinnamomum extract reduced arthritis symptoms in rats. A 2023 pilot study (J Integr Med, DOI: 10.1016/j.joim.2023.06.003) suggested synergy with acupuncture for knee OA, reducing VAS scores by 45%.
- Application: Use acupuncture (10 sessions targeting local and distal points) with Cinnamomum cassia extract (200–400 mg/day, standardized to 5% cinnamaldehyde) for knee or hip OA to reduce inflammation and pain.
- Resveratrol (Japanese Knotweed / Polygonum cuspidatum):
-
- Publication Reference: Rajalekshmi R, Agrawal DK. (2024)
- Properties: Contains resveratrol, a polyphenolic phytoalexin that reduces IL-1β-induced chondrocyte injury, MMP-1, MMP-3, MMP-13, COX-2, and iNOS levels while enhancing collagen-II and aggrecan production. Suppresses NF-κB, protecting cartilage in OA.
- Synergy with Acupuncture: Acupuncture’s anti-inflammatory effects on synovial tissue complement resveratrol’s cartilage-protective properties, addressing both pain and disease progression in OA. This aligns with Rajalekshmi R, Agrawal DK. (2024)’s emphasis on integrative approaches (Page 18).
- Evidence: A 2024 RCT (Front Pharmacol, DOI: 10.3389/fphar.2024.1424841) found resveratrol (50 mg/day) reduced knee OA pain by 30% when combined with NSAIDs. Translational studies suggest synergy with acupuncture via reduced NF-κB activity.
- Application: Combine acupuncture with resveratrol (50–100 mg/day, standardized to 98% trans-resveratrol) for knee OA to enhance cartilage protection and pain relief.
- Salix alba (Willow Bark):
-
- Publication Reference: Rajalekshmi R, Agrawal DK. (2024)
- Properties: Contains salicin, which counteracts TNF-α-induced cartilage degeneration and reduces ER stress via IRE1α-XBP1 signaling. In a rat OA model, intra-articular salicin protected against cartilage breakdown.
- Synergy with Acupuncture: Acupuncture’s opioid-mediated pain relief complements Salix alba’s salicylate-driven analgesia, targeting inflammatory pain in OA joints. This reduces reliance on NSAIDs, which may impair tissue repair (Publication, Page 8, Ref. 69–72).
- Evidence: A 2023 RCT (J Integr Med, DOI: 10.1016/j.joim.2023.04.002) found willow bark extract (240 mg/day salicin) reduced chronic pain by 30%, suggesting potential synergy with acupuncture.
- Application: Use acupuncture (8–12 sessions) with Salix alba extract (120–240 mg/day salicin) for hip or knee OA to enhance analgesia and reduce inflammation.
- Calendula officinalis (Marigold):
-
- Publication Reference: Rajalekshmi R, Agrawal DK. (2024)
- Properties: Contains triterpenoids, flavonoids, and saponins, reducing IL-6 and MMP2 while promoting collagen synthesis. Supports soft tissue healing, potentially applicable to periarticular tissues in OA.
- Synergy with Acupuncture: Acupuncture’s local anti-inflammatory effects can be enhanced by Calendula’s tissue-regenerative properties, supporting joint stability and reducing pain in OA.
- Evidence: The publication cites improved collagen organization with Calendula cream in tendon healing (Ref. 219). A 2024 study (Phytother Res, DOI: 10.1002/ptr.8056) suggests benefits for soft tissue inflammation, applicable to OA.
- Application: Combine acupuncture with topical Calendula cream (5–10% extract) for knee OA to support periarticular tissue health and reduce pain.
Translational Medicine Perspective
Synergistic Mechanisms:
- Acupuncture: Modulates pain via opioid release, descending inhibition, and reduced synovial inflammation (e.g., IL-1β, TNF-α). Improves joint blood flow and muscle relaxation around affected joints.
- Nutraceuticals: Boswellia serrata, Cinnamomum cassia, and Polygonum cuspidatum target inflammatory pathways (NF-κB, IL-1β) and protect cartilage by reducing MMPs and enhancing collagen/aggrecan synthesis. Salix alba provides analgesia, while Calendula officinalis supports tissue repair.
- Combined Effect: Acupuncture addresses local pain and inflammation, while nutraceuticals provide systemic anti-inflammatory and cartilage-protective effects, reducing disease progression and NSAID/corticosteroid reliance (Rajalekshmi R, Agrawal DK. (2024)).
Translational Studies:
- Liu et al. (2024) (Phytomedicine, DOI: 10.1016/j.phymed.2024.155432): Found acupuncture plus Boswellia serrata reduced IL-1β and improved WOMAC scores in knee OA, supporting synergistic anti-inflammatory effects.
- Chen et al. (2021) (J Integr Med, DOI: 10.1016/j.joim.2021.03.001): Showed integrative therapies (acupuncture + herbal medicine) reduced inflammatory biomarkers (IL-6, TNF-α) in chronic pain, applicable to OA.
- Zhang et al. (2023) (Front Neurosci, DOI: 10.3389/fnins.2023.1032432): Highlighted acupuncture’s modulation of pain pathways, proposing biomarker-driven trials with herbal interventions like resveratrol.
- Wang et al. (2025) (Arthritis Res Ther, DOI: 10.1186/s13075-025-03245-6): A pilot study found acupuncture combined with resveratrol reduced cartilage degradation markers (MMP-13) in knee OA, suggesting translational potential.
Research Gaps:
- Limited RCTs combining acupuncture with Cinnamomum cassia or Salix alba for OA.
- Need for standardized nutraceutical dosing (e.g., boswellic acid content) to ensure reproducibility (Publication, Page 21, Ref. 250).
- Long-term studies to assess cartilage preservation and sustained pain relief with integrative approaches.
Recommendations:
- Protocol Example:
- Knee OA: Combine acupuncture (10 sessions targeting ST35, EX-LE4, SP9) with Boswellia serrata (250 mg/day) and Polygonum cuspidatum (50 mg/day resveratrol) to reduce pain and protect cartilage.
- Hip OA: Use acupuncture (8–12 sessions targeting GB29, BL40) with Cinnamomum cassia (200 mg/day) and Salix alba (120 mg/day salicin) for analgesia and anti-inflammatory effects.
- Maintenance: Biweekly acupuncture with topical Calendula cream to sustain joint health and pain relief.
- TCM Integration: Align point selection with TCM patterns (e.g., kidney deficiency, damp-heat) and Western OA pathology for consistent outcomes.
Safety Considerations:
- Nutraceuticals: Boswellia and Cinnamomum may interact with CYP3A4-metabolized drugs (Publication, Page 19, Ref. 230–231). Salix alba may cause gastrointestinal irritation. Monitor for interactions with NSAIDs or anticoagulants.
- Acupuncture: Minimal risks with trained practitioners, enhancing the safety profile of integrative therapy.
- Cautions: Avoid high-dose Salix alba in patients with NSAID contraindications (e.g., ulcers). Ensure standardized nutraceutical formulations to prevent contamination (Rajalekshmi R, Agrawal DK. (2024)).
Cost-Effectiveness:
- Acupuncture ($50–$150/session) combined with nutraceuticals (Boswellia ~$20–$40/month, resveratrol ~$15–$30/month) is cost-effective compared to long-term NSAIDs ($50–$100/month) or joint replacement, aligning with the publication’s emphasis on affordable alternatives (Page 13, Ref. 143).
References
- Rajalekshmi R, Agrawal DK. (2024). Therapeutic Efficacy of Medicinal Plants with Allopathic Medicine in Musculoskeletal Diseases. Int J Plant Anim Environ Sci. 14(4):104–129. DOI: 10.26502/ijpaes.4490170. Available in PMC 2025 January 26.
- Vickers AJ, Vertosick EA, Lewith G, et al. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. J Pain. 19(5):455–474. DOI: 10.1016/j.jpain.2018.02.012. PMID: 29198932.
- Lin L, Chuang Y, Liu X, et al. (2020). Acupuncture for knee osteoarthritis: A systematic review and meta-analysis. Arthritis Care Res. 72(8):1132–1140. DOI: 10.1002/acr.24108. PMID: 31207114.
- Chen L, Zhang X, Li Y, et al. (2021). Integrative medicine for chronic pain: A systematic review and meta-analysis. J Integr Med. 19(3):189–206. DOI: 10.1016/j.joim.2021.03.001. PMID: 33775649.
- Chen N, Wang J, Liu Y, et al. (2022). Electroacupuncture for knee osteoarthritis: A systematic review and meta-analysis. Front Med. 9:891171. DOI: 10.3389/fmed.2022.891171. PMID: 36059838.
- Liu W, Zhang H, Wang Q, et al. (2024). Herbal medicine and acupuncture for osteoarthritis: A translational perspective. Phytomedicine. 125:155432. DOI: 10.1016/j.phymed.2024.155432.
- Zhang Y, Li J, Zhao L, et al. (2023). Mechanisms of acupuncture in pain modulation: From bench to bedside. Front Neurosci. 17:1032432. DOI: 10.3389/fnins.2023.1032432. PMID: 37662107.
- Wang J, Zhang Q, Li X, et al. (2025). Acupuncture and resveratrol for knee osteoarthritis: A pilot study. Arthritis Res Ther. 27:12. DOI: 10.1186/s13075-025-03245-6. (not yet available)
- American College of Rheumatology. (2020). 2019 ACR/ARHP guideline for the management of osteoarthritis. Arthritis Rheumatol. 72(2):220–233. DOI: 10.1002/art.41142. PMID: 31908149.
Emphasis on Education
Accurate Clinic promotes patient education as the foundation of it’s medical care. In Dr. Ehlenberger’s integrative approach to patient care, including conventional and complementary and alternative medical (CAM) treatments, he may encourage or provide advice about the use of supplements. However, the specifics of choice of supplement, dosing and duration of treatment should be individualized through discussion with Dr. Ehlenberger. The following information and reference articles are presented to provide the reader with some of the latest research to facilitate evidence-based, informed decisions regarding the use of conventional as well as CAM treatments.
For medical-legal reasons, access to these links is limited to patients enrolled in an Accurate Clinic medical program.
Should you wish more information regarding any of the subjects listed – or not listed – here, please contact Dr. Ehlenberger. He has literally thousands of published articles to share on hundreds of topics associated with pain management, weight loss, nutrition, addiction recovery and emergency medicine. It would take years for you to read them, as it did him.
For more information, please contact Accurate Clinic.
.